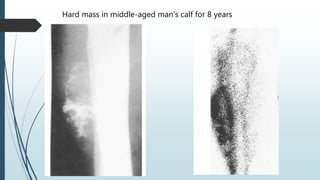
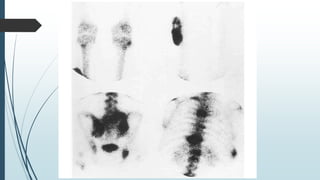
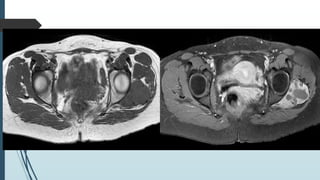
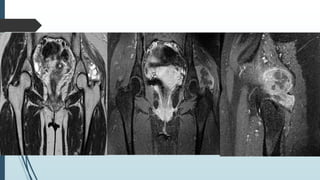
This document discusses two types of soft tissue sarcomas: mesenchymal chondrosarcoma and synovial sarcoma. Both tumor types contain soft tissue components, calcified areas, mineralization, and cystic areas or necrosis/hemorrhage. Mesenchymal chondrosarcoma has a bimodal age distribution in the 3rd and 5th decades, while synovial sarcoma typically presents between 15-50 years of age, with a mean of 35 years. The tumors can arise in soft tissues near joints. Imaging findings include soft tissue masses with mineralization or calcification that demonstrate enhancement. Histopathological examination is needed for definitive diagnosis of each tumor type.