Downloaded 193 times
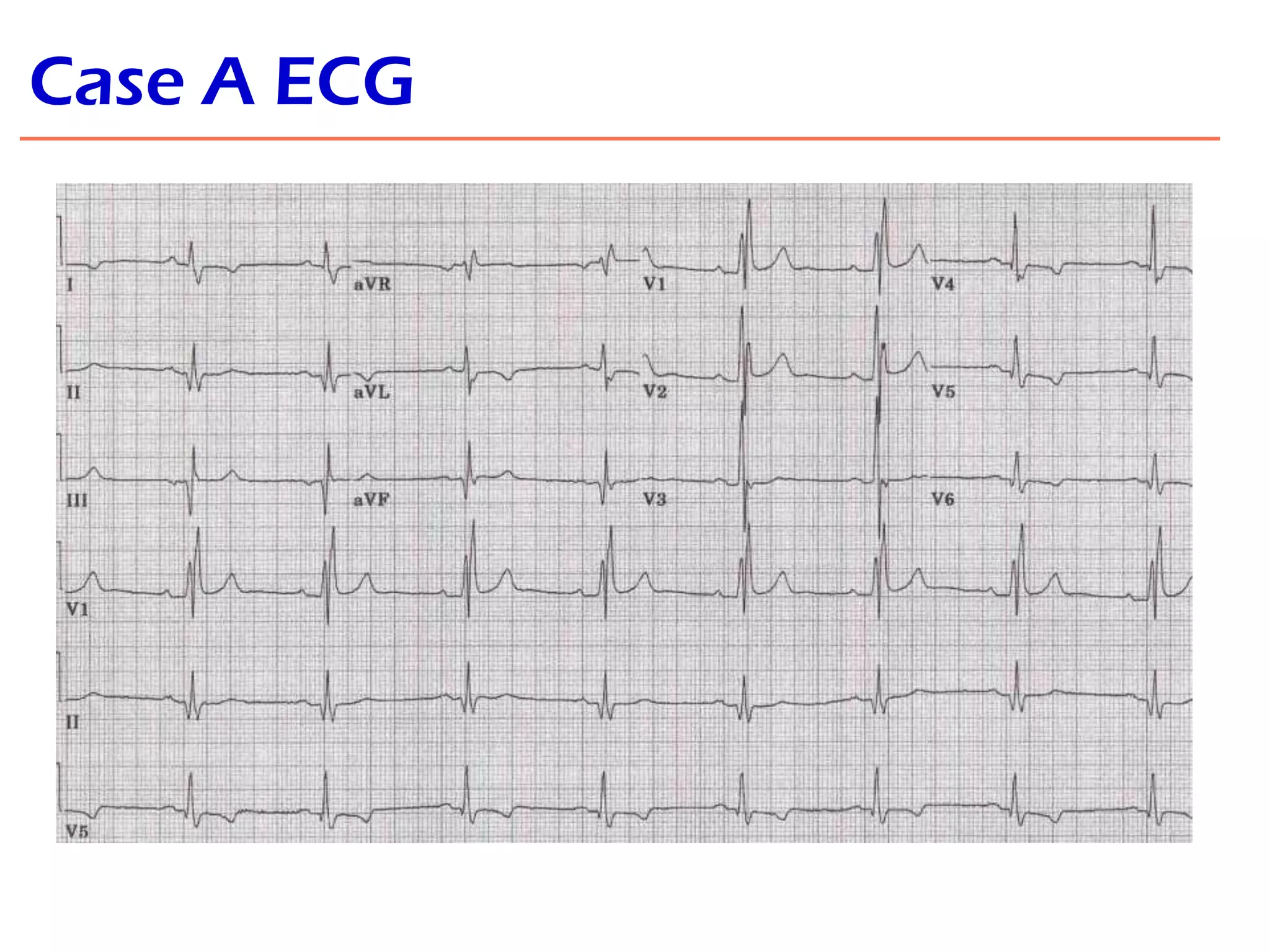


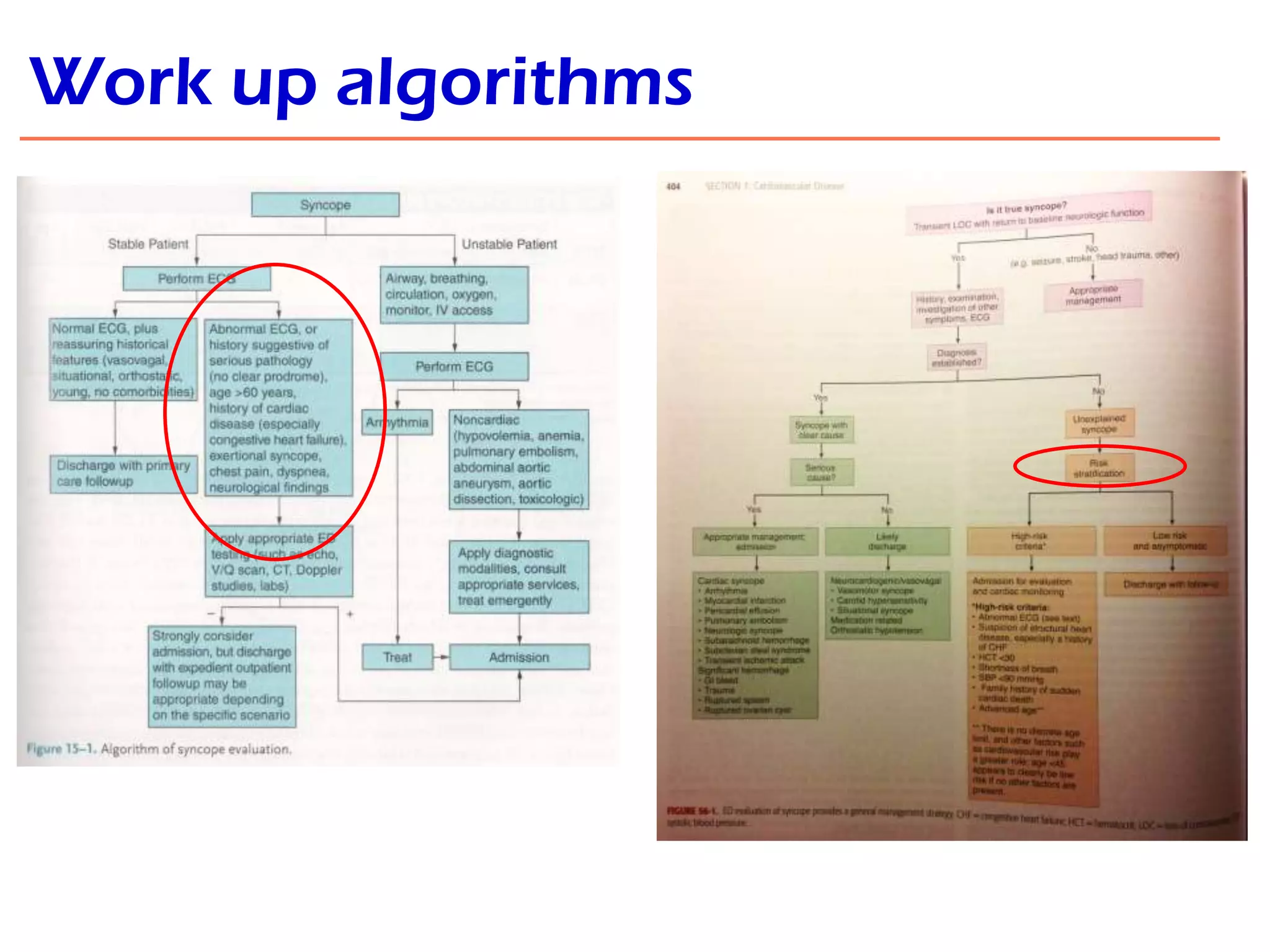
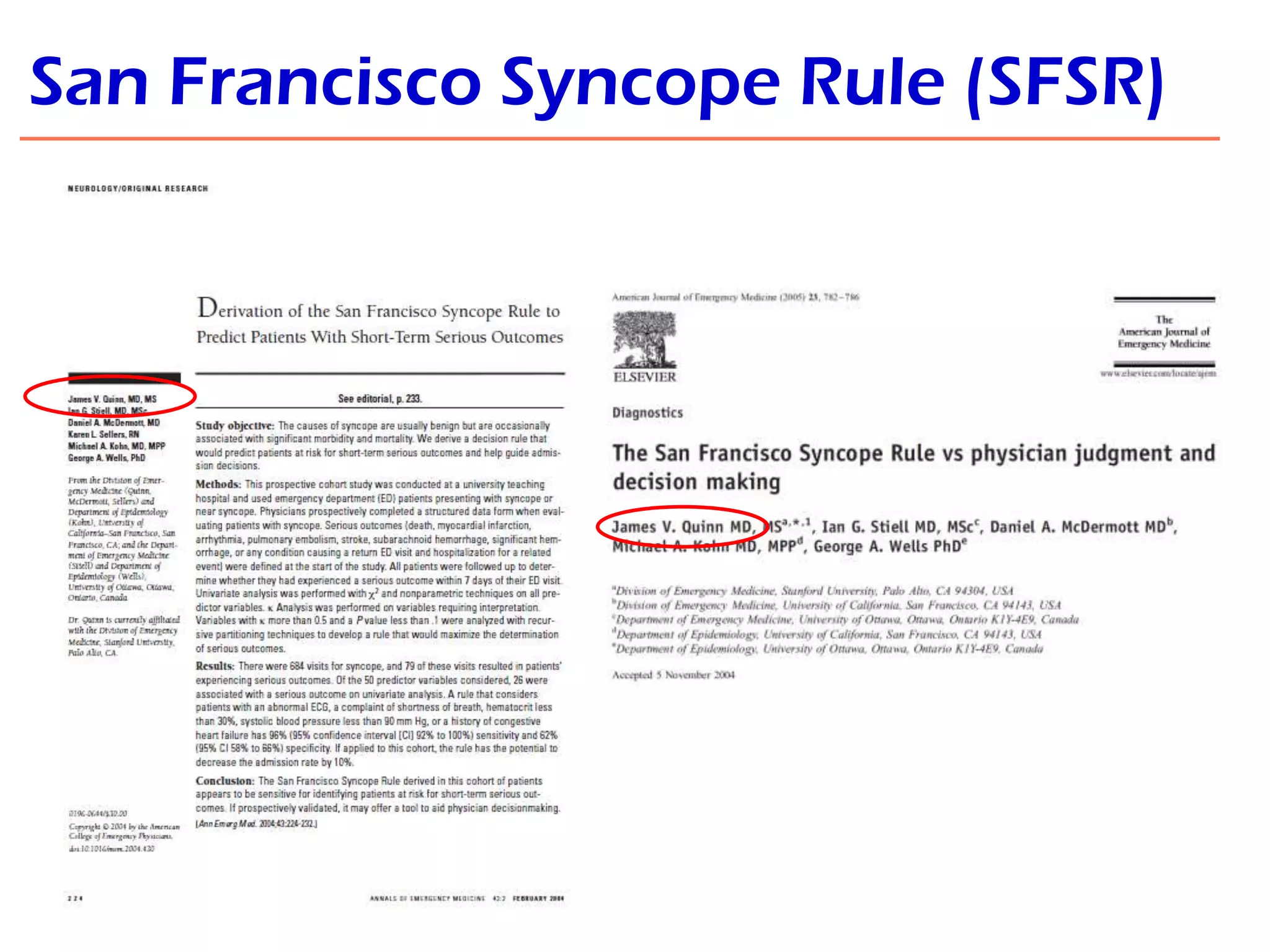
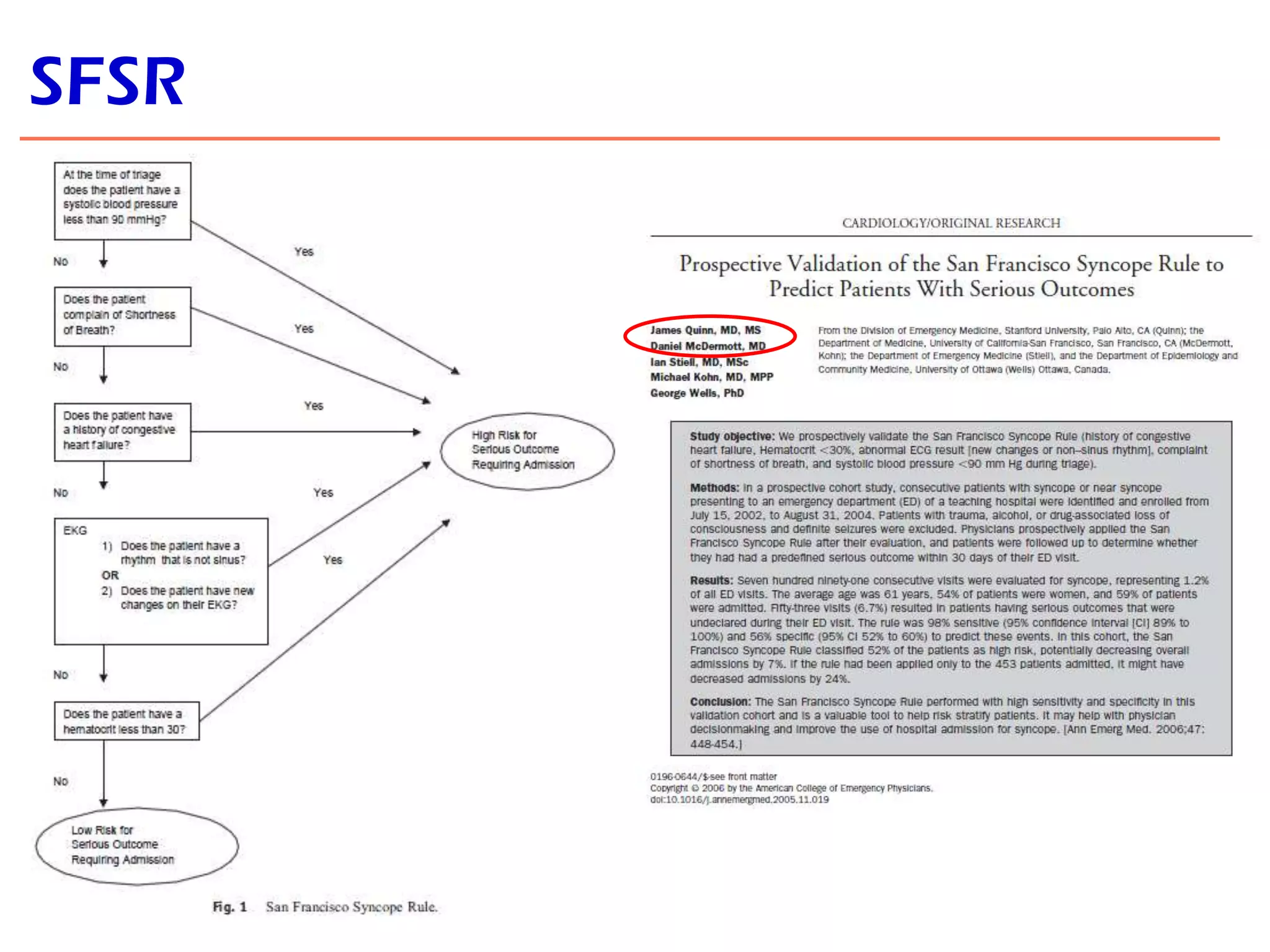
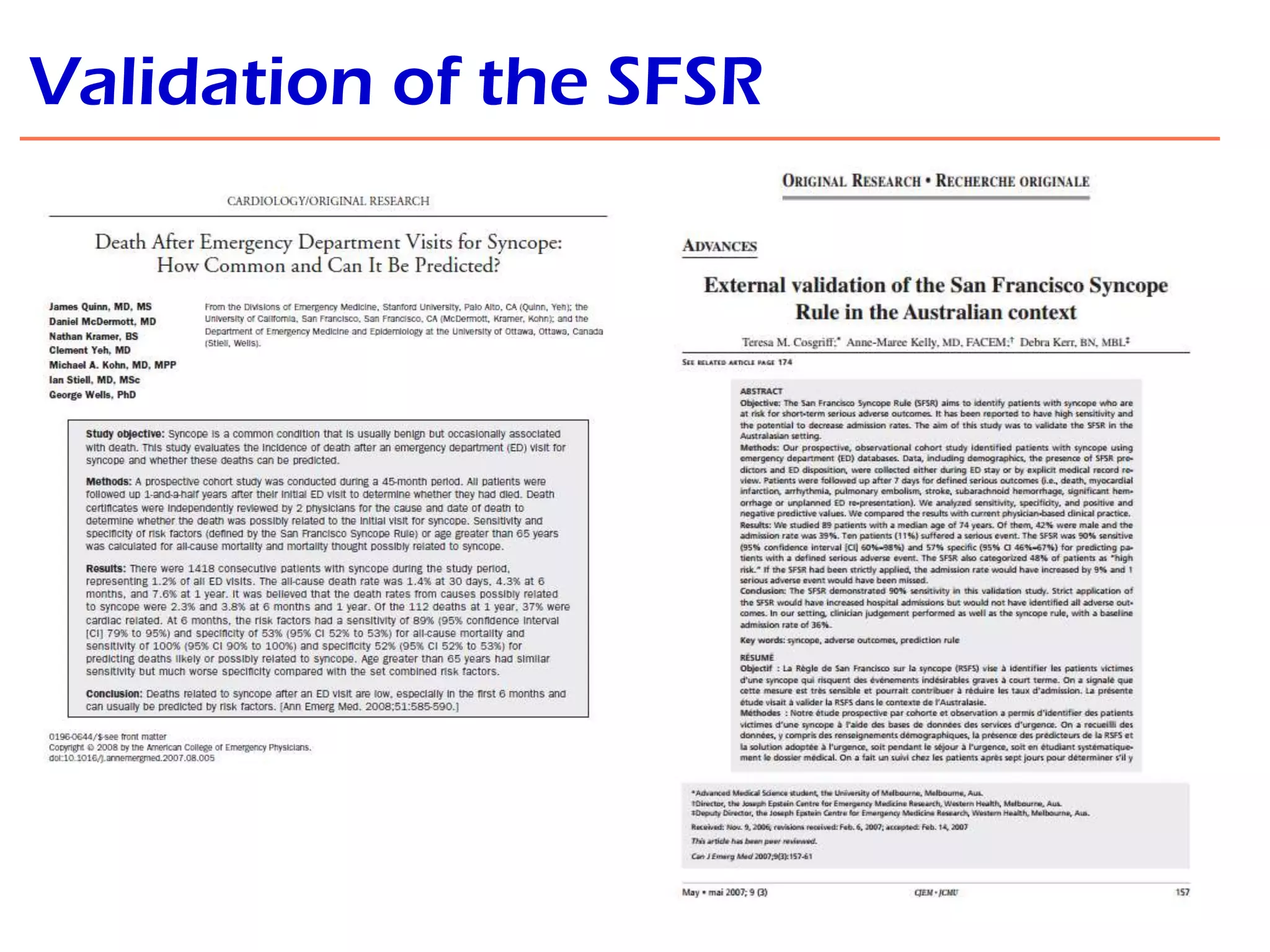
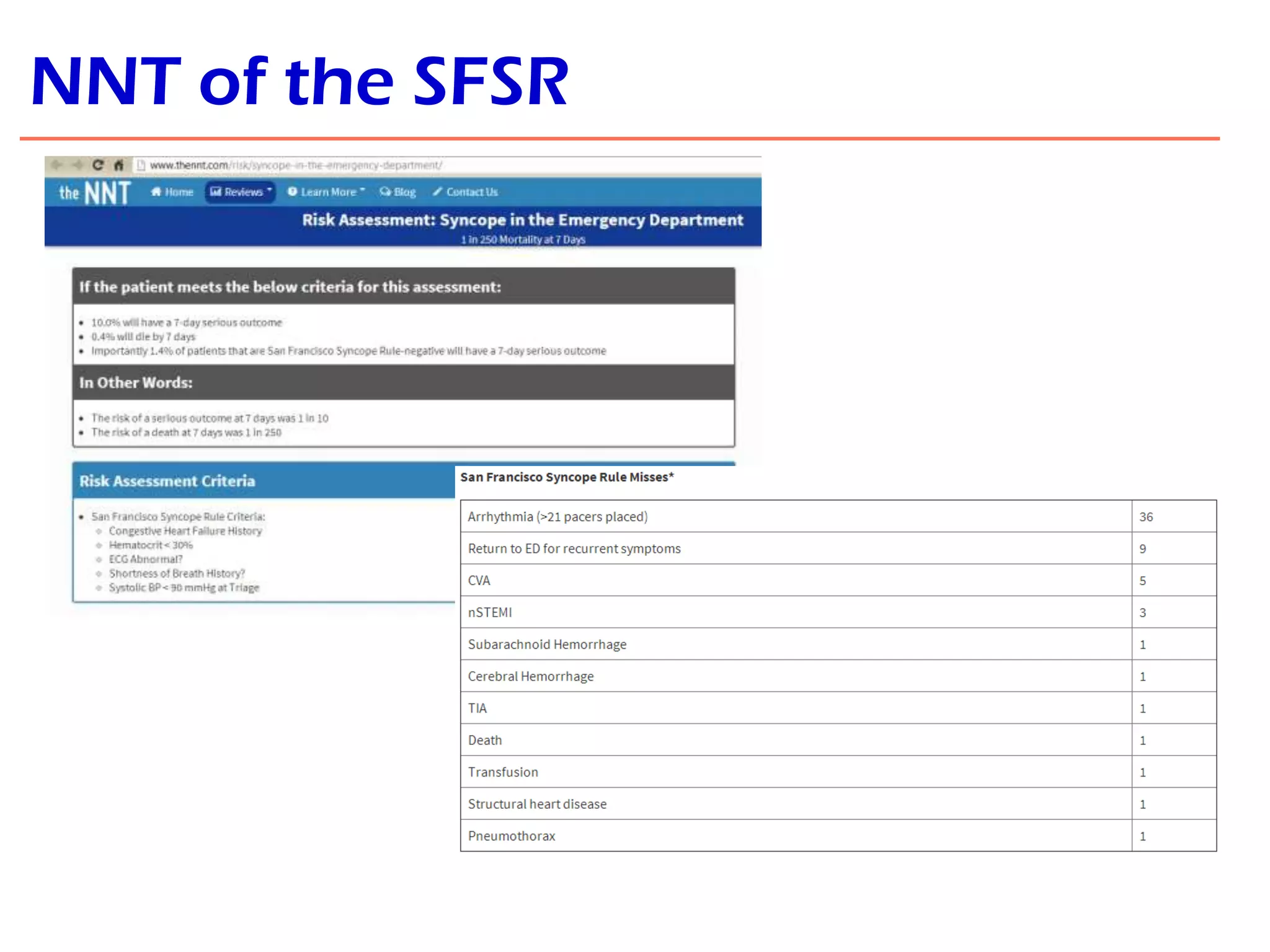
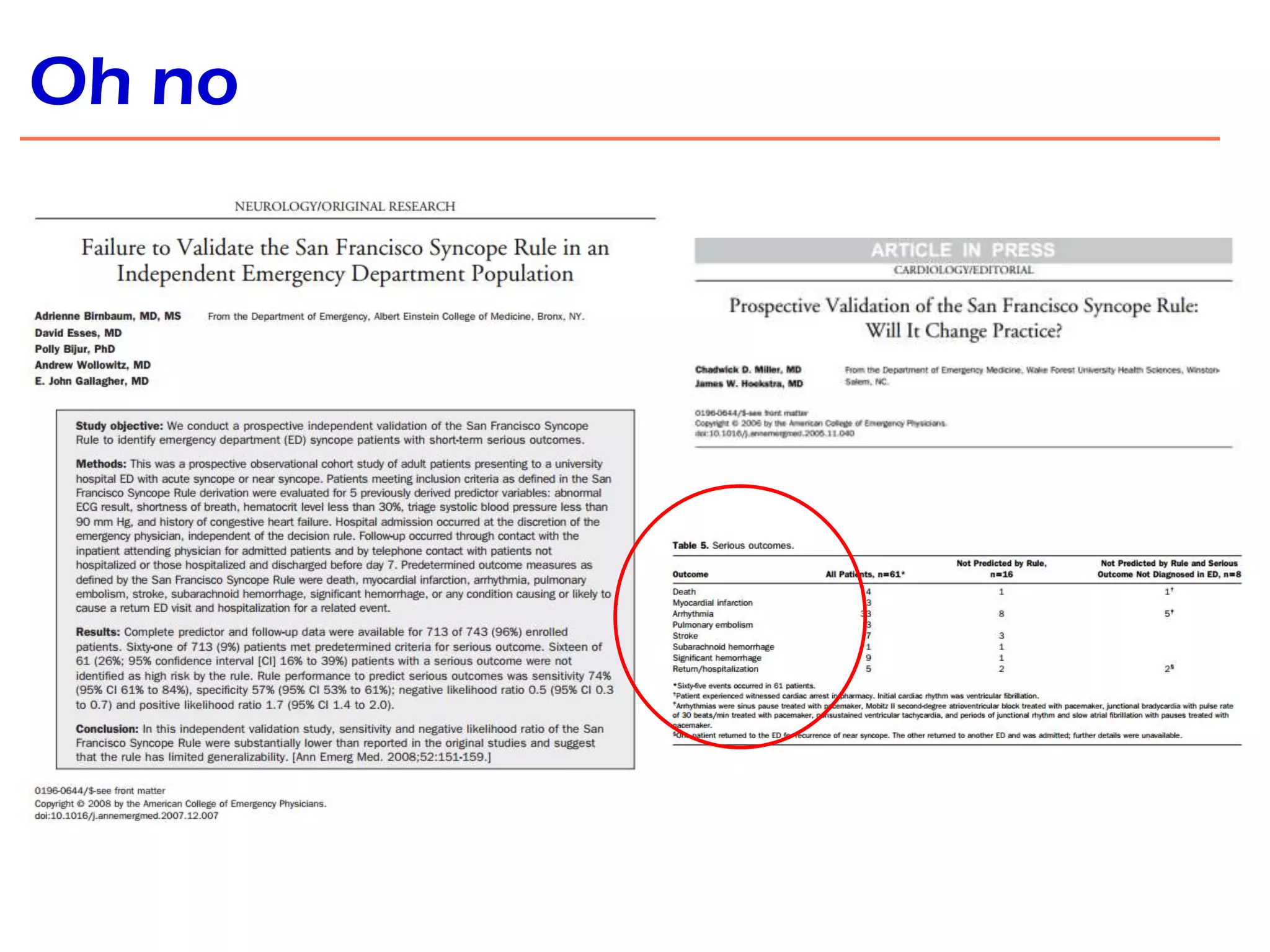
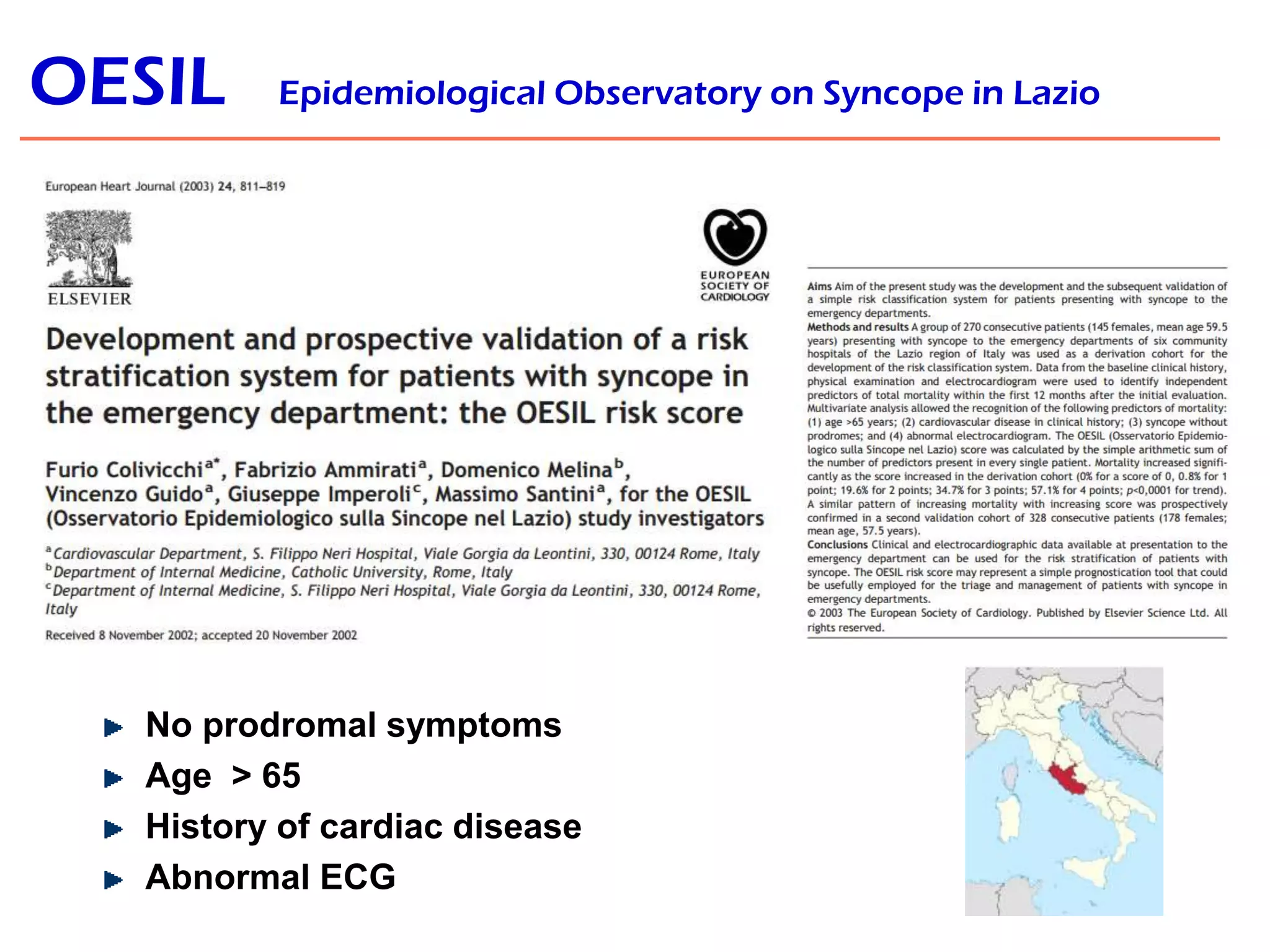
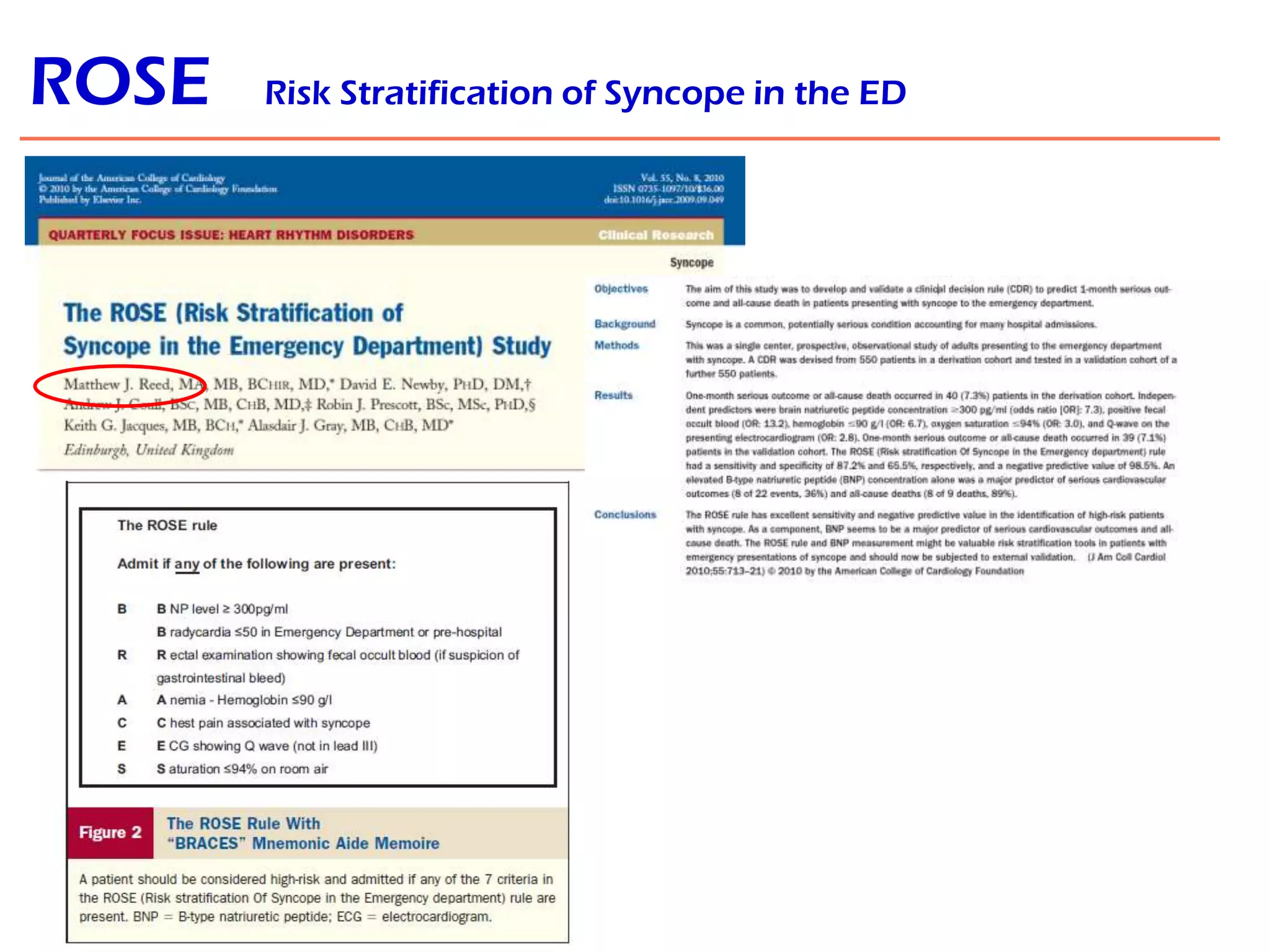
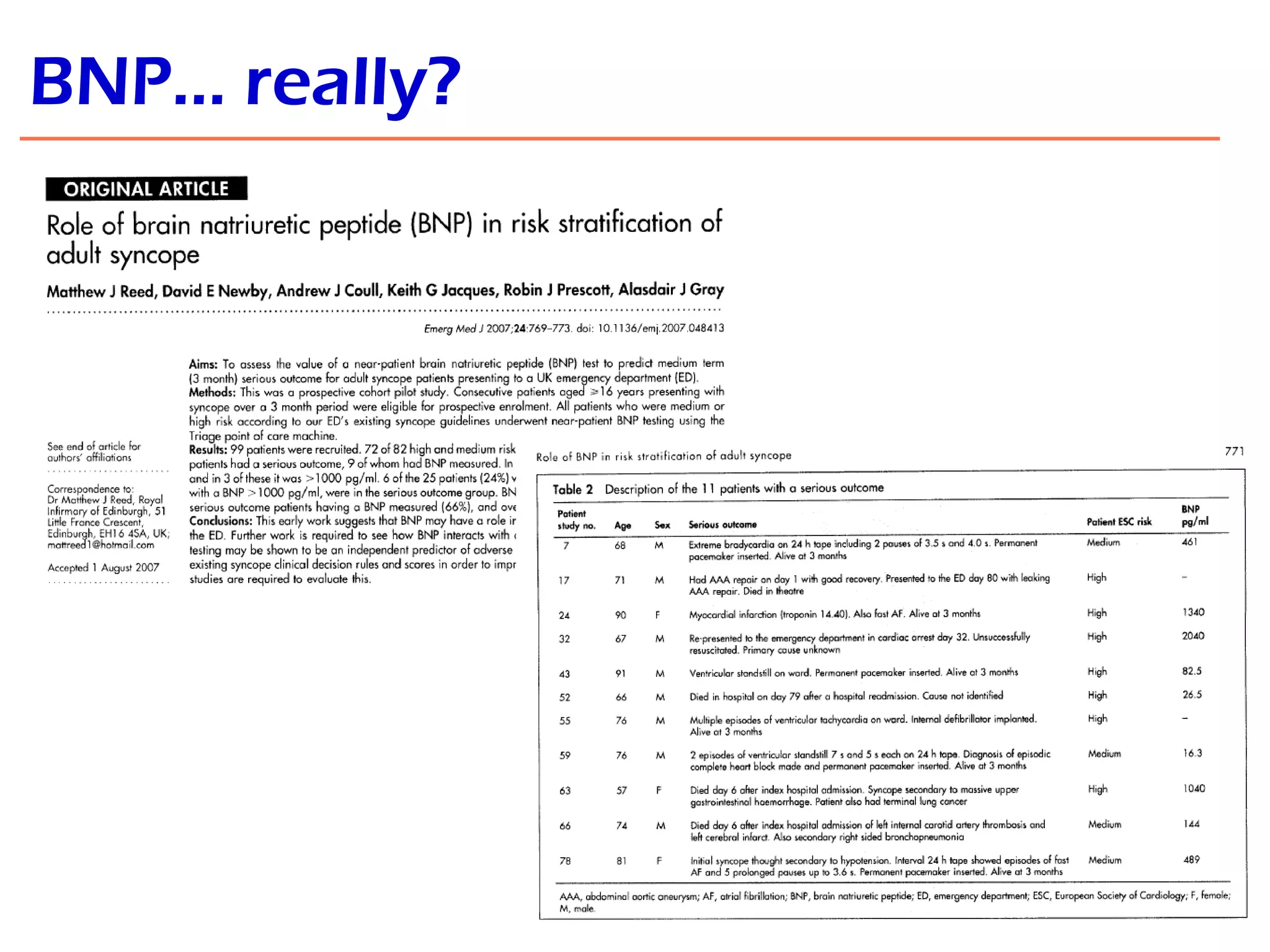
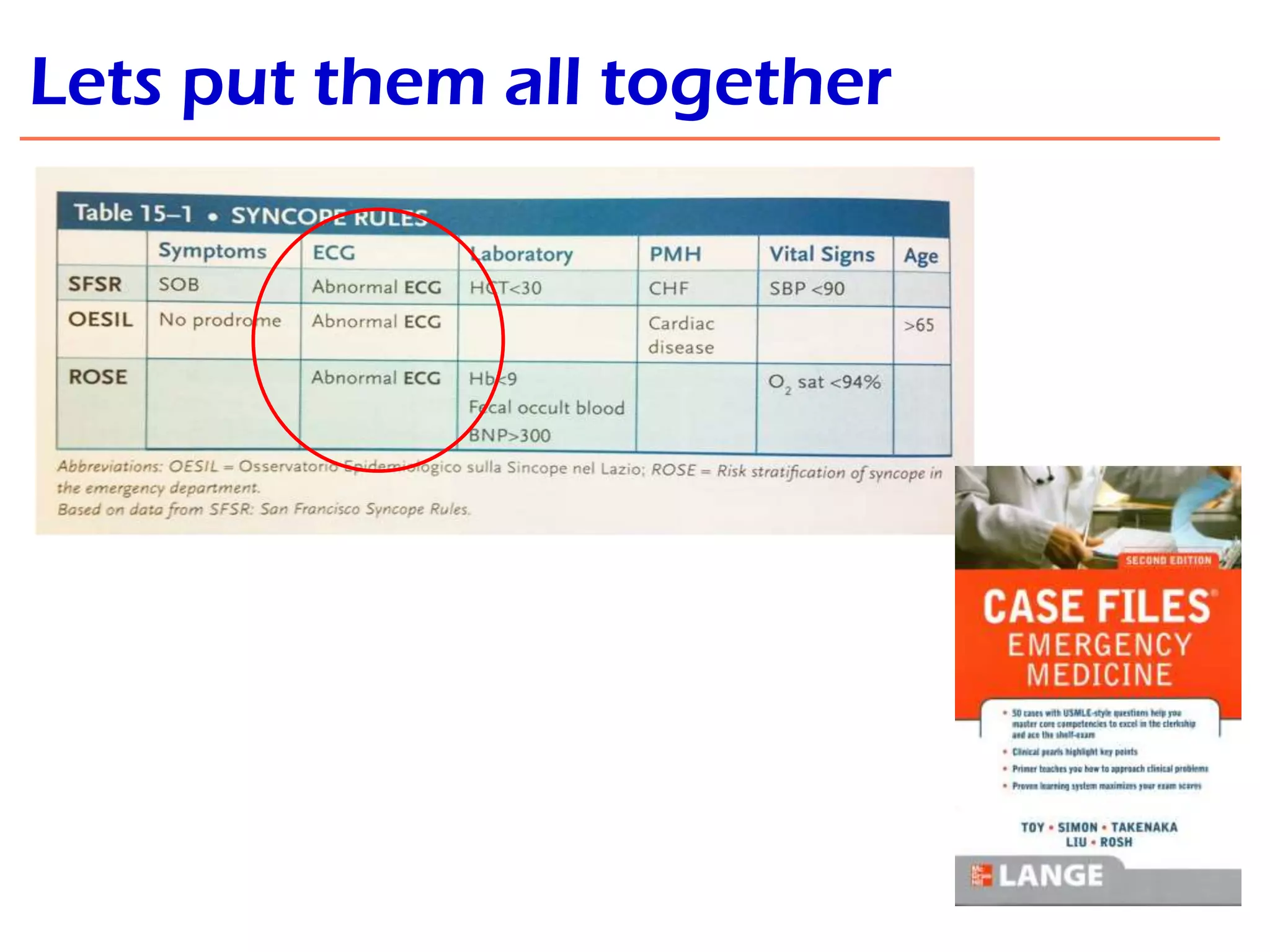
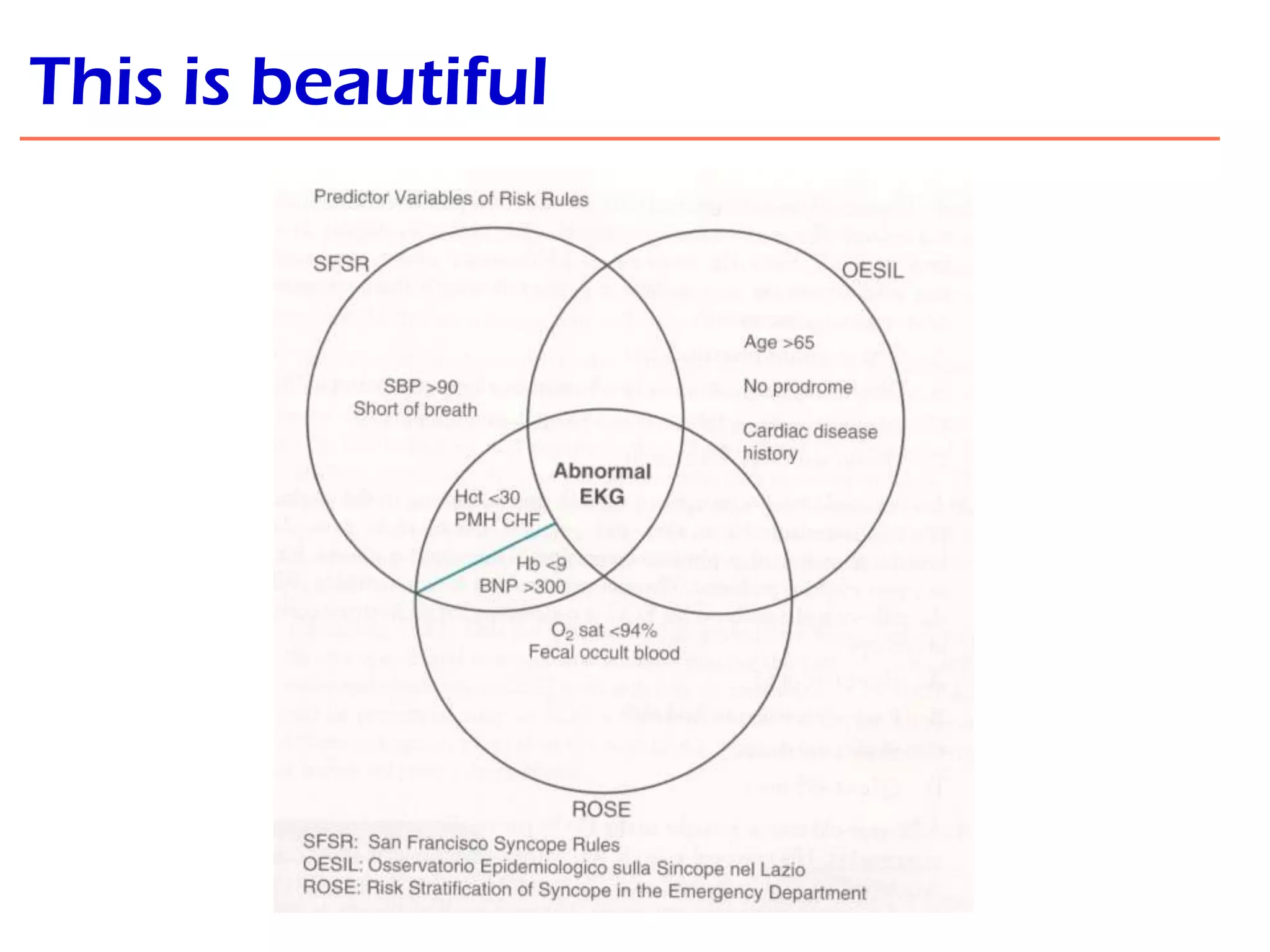

This document contains a presentation on the assessment of syncope given to registrars at an emergency department teaching meeting. It includes two case presentations of patients who presented with syncope, along with their ECG readings, and a discussion of the differential diagnosis, evaluation algorithms, and decision rules that can be used to evaluate syncope, including the San Francisco Syncope Rule, OESIL criteria, and ROSE risk stratification. The presenter encourages questions and discussion from the audience on syncope evaluation and interesting ECG findings.

































































































![Apporach to lung biopsy [Auto-saved].pptx latest](https://cdn.slidesharecdn.com/ss_thumbnails/apporachtolungbiopsyauto-saved-251211225655-93258539-thumbnail.jpg?width=640&height=640&fit=bounds)









