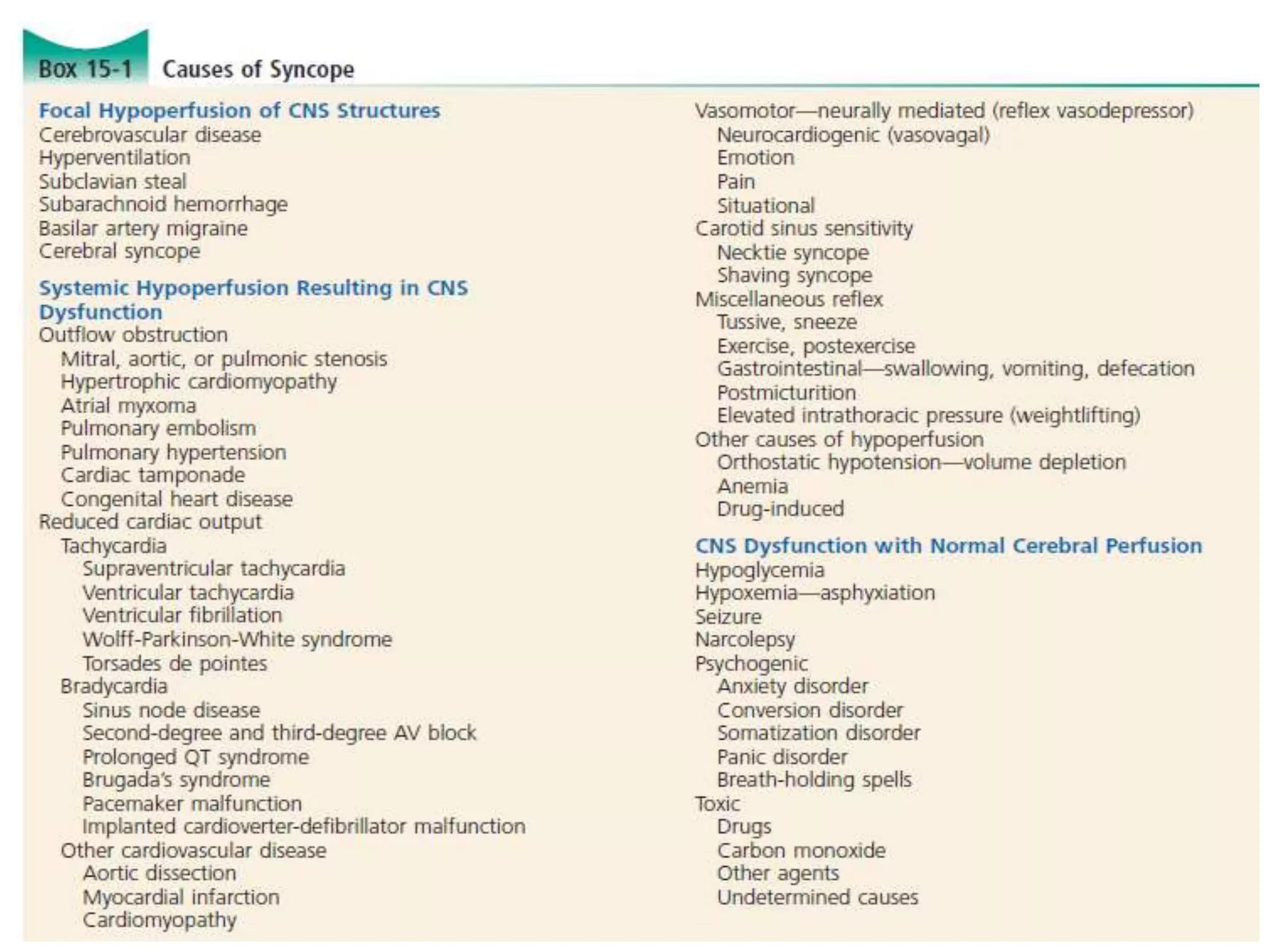
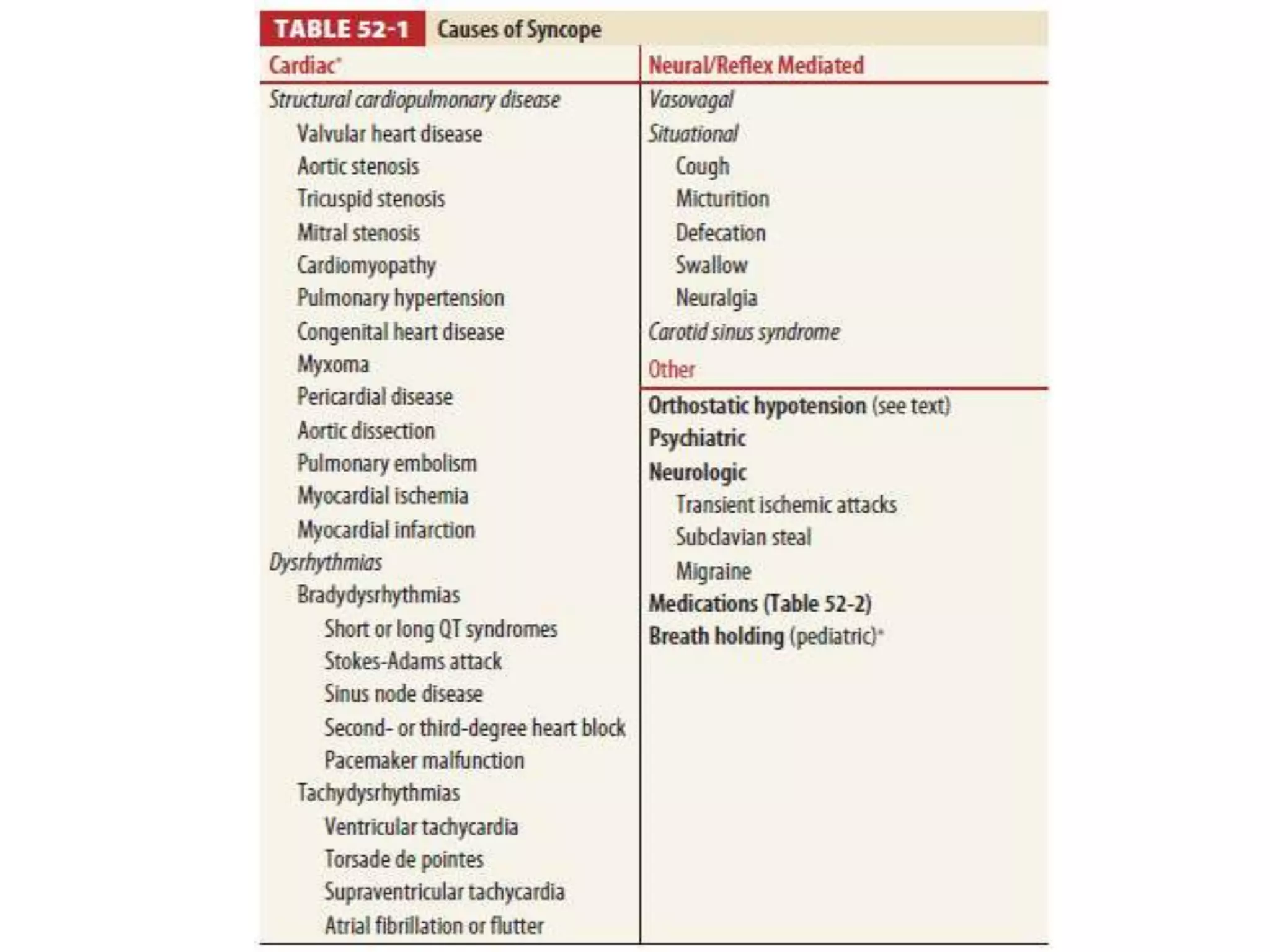
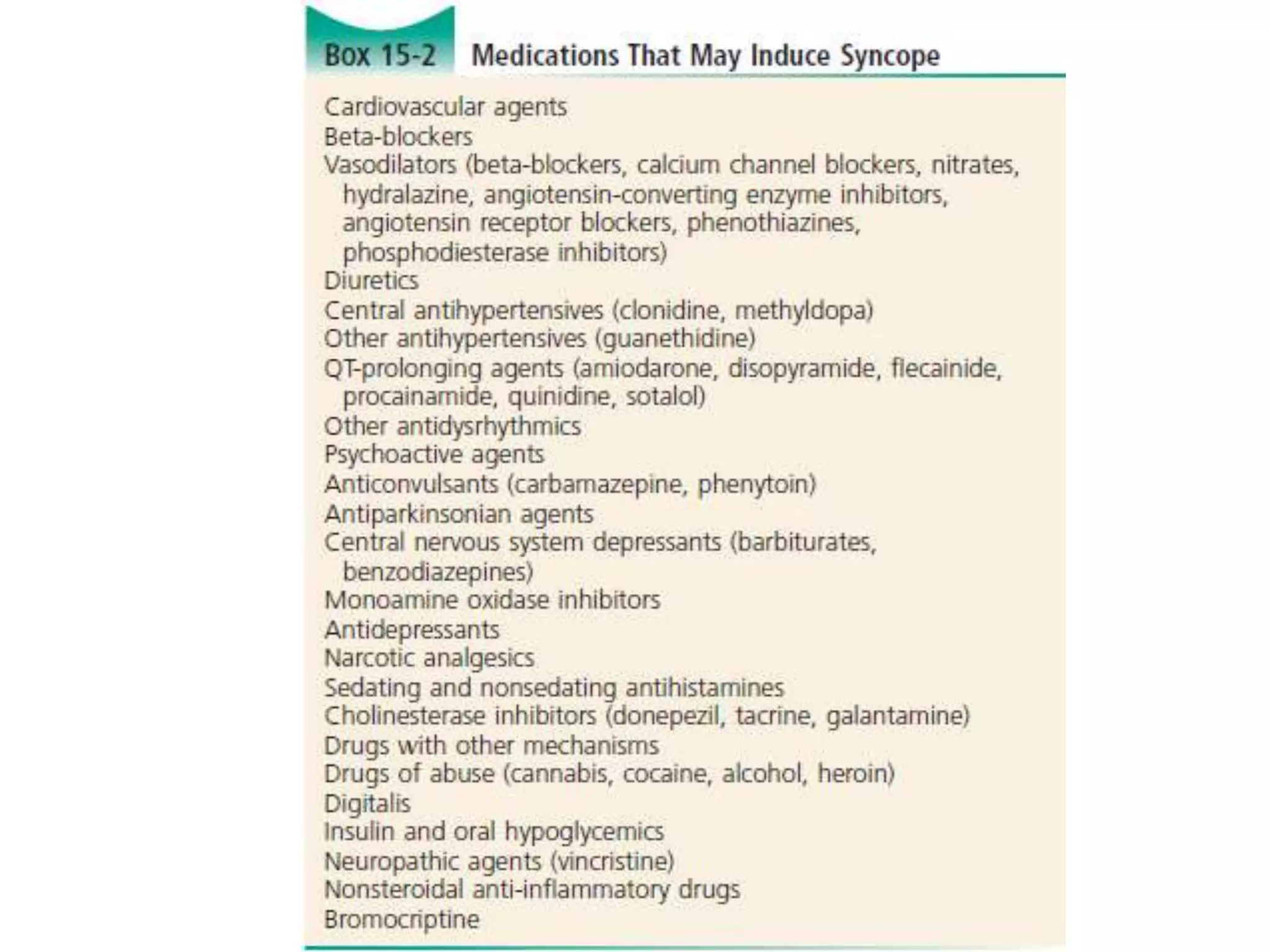
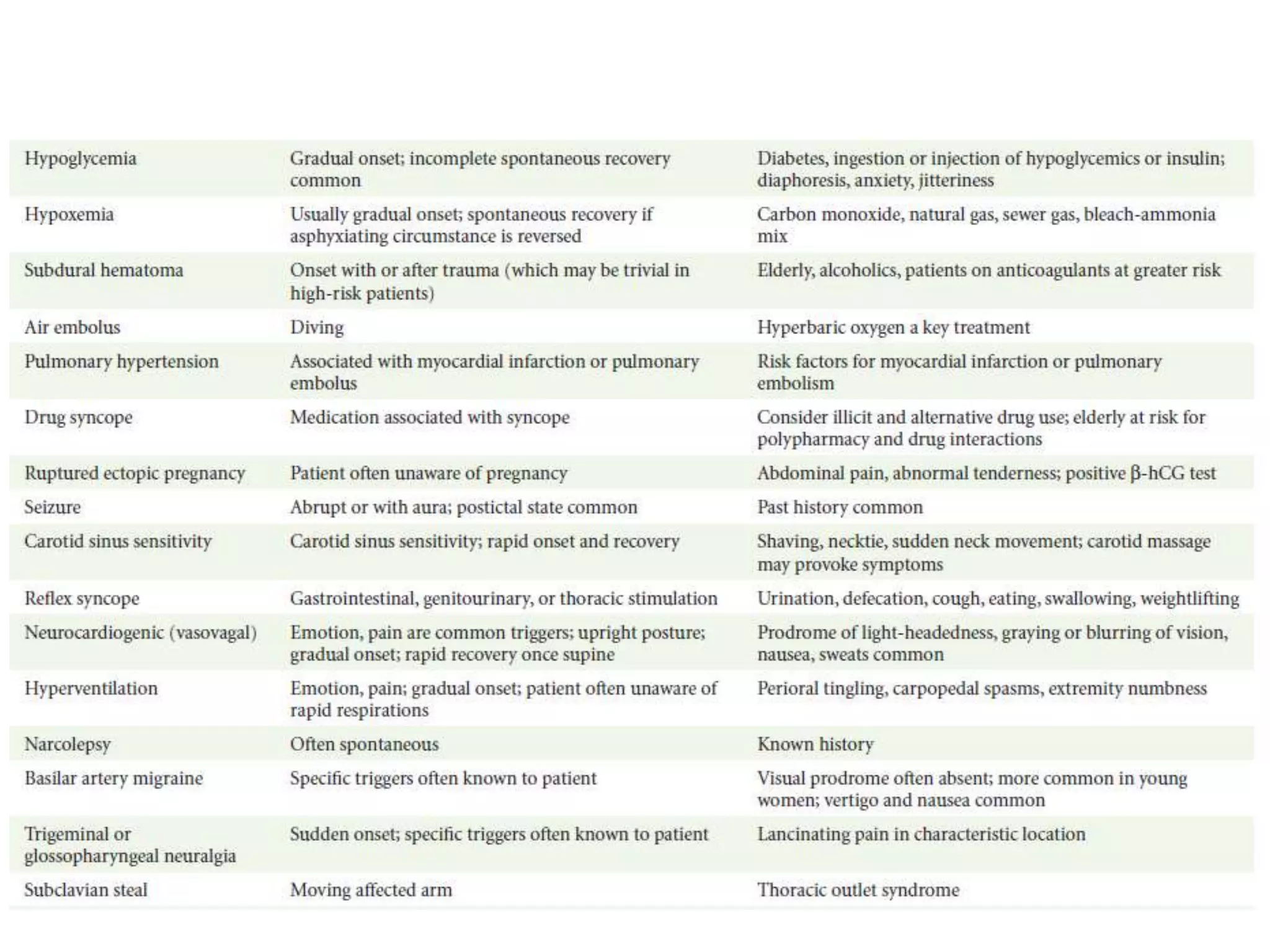
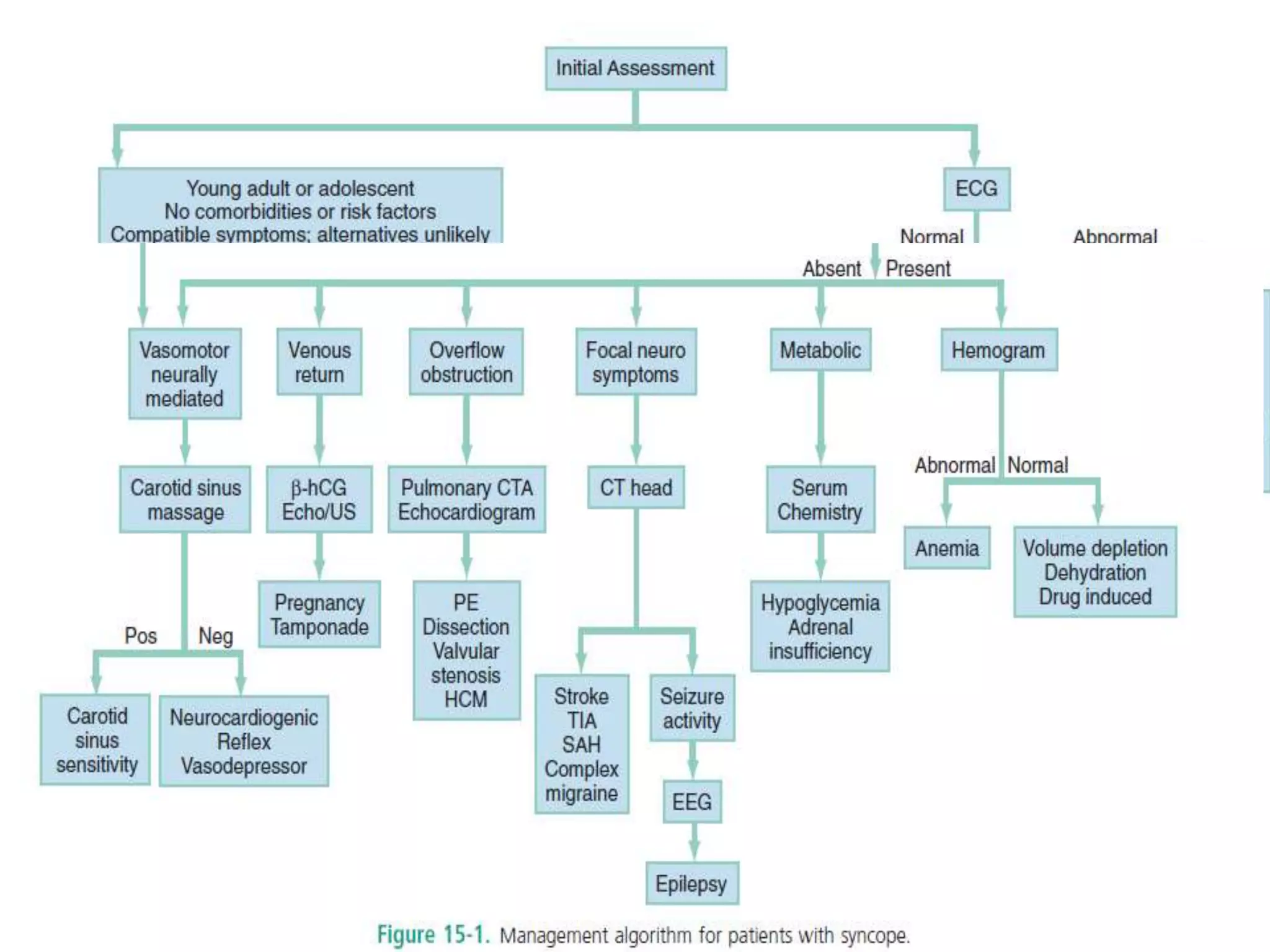
Syncope, or fainting, is defined as a transient loss of consciousness associated with loss of postural tone that resolves spontaneously. It accounts for 0.8% of ED visits and has a prevalence of 19% in the general population. Common causes include vasovagal, cardiac, orthostatic, and medication-related reactions. A thorough history and physical exam can suggest a diagnosis in 45% of cases and help determine appropriate disposition, whether inpatient for high-risk patients or outpatient follow up for low-risk cases.