





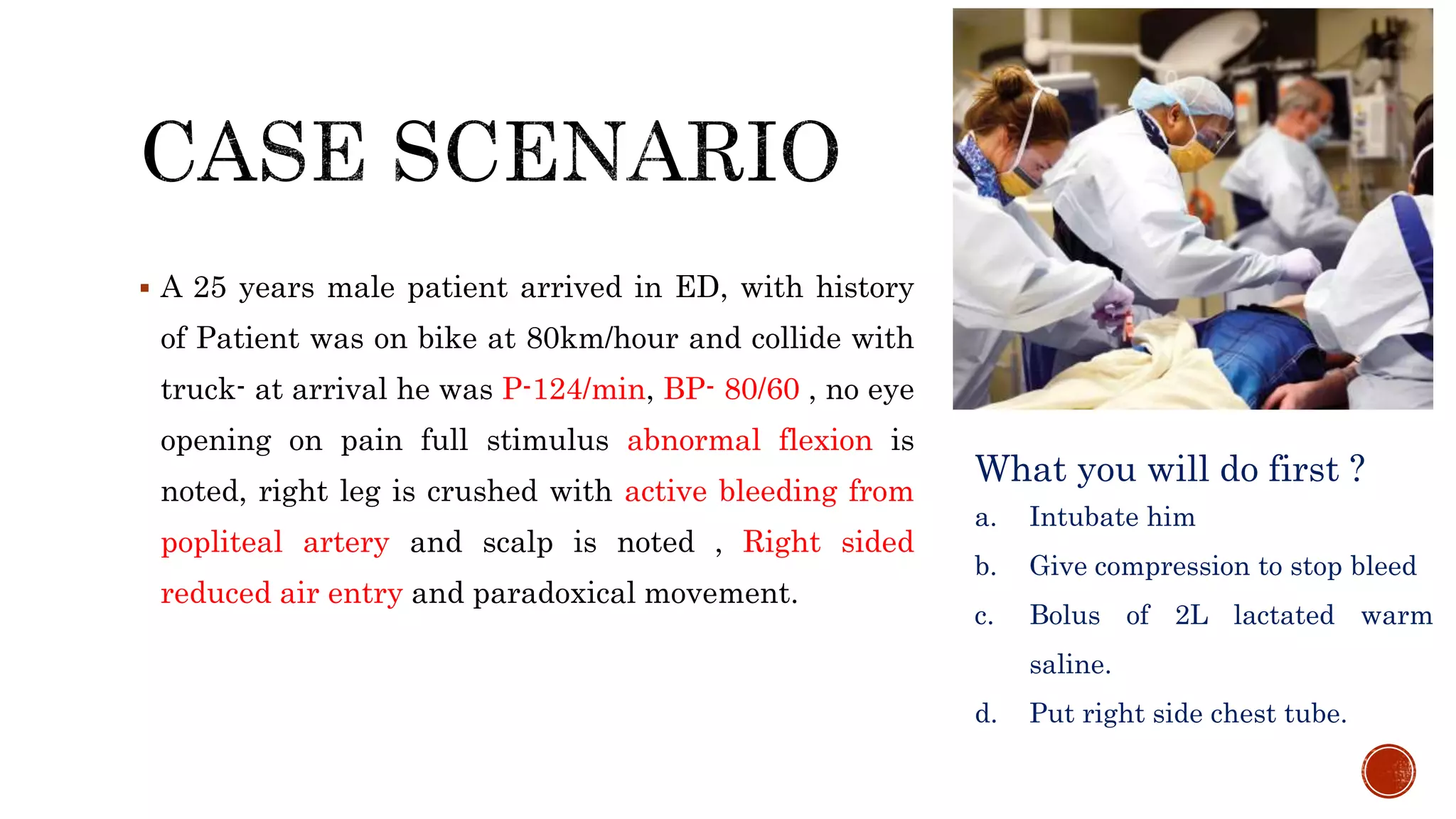








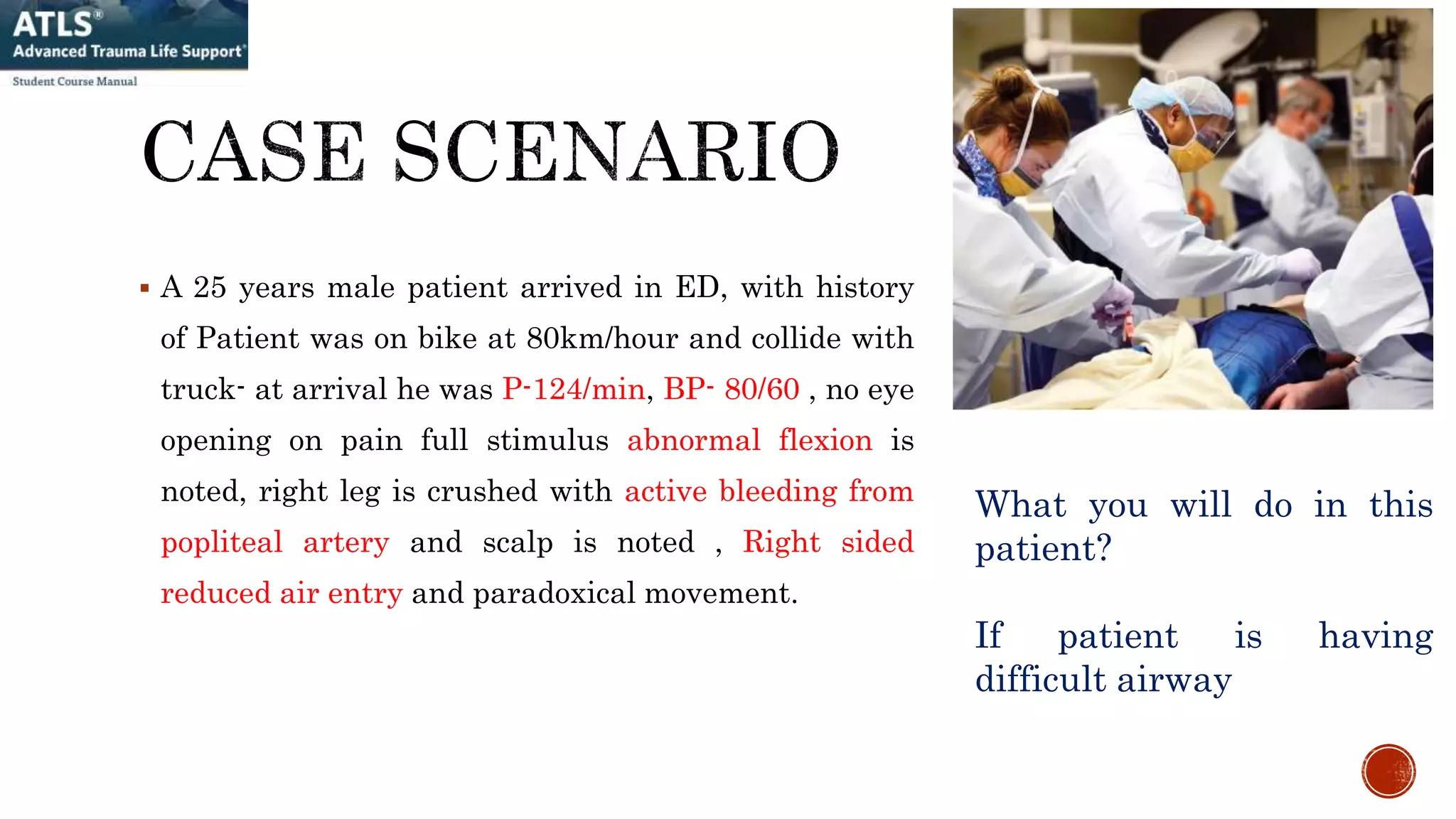


























1. A 25-year-old male patient arrived at the ED after a motorcycle collision with signs of airway compromise, reduced breathing, and bleeding requiring immediate intubation, chest tube placement, and fluid resuscitation to address life-threatening injuries. 2. Management of major trauma involves a primary survey addressing the immediate ABCDE threats with airway control, breathing support, hemorrhage control, and disability assessment as the highest priorities. 3. Burn management similarly focuses first on securing the airway, assessing for inhalation injury, and aggressively resuscitating to prevent shock from ongoing fluid losses through the burned skin.
































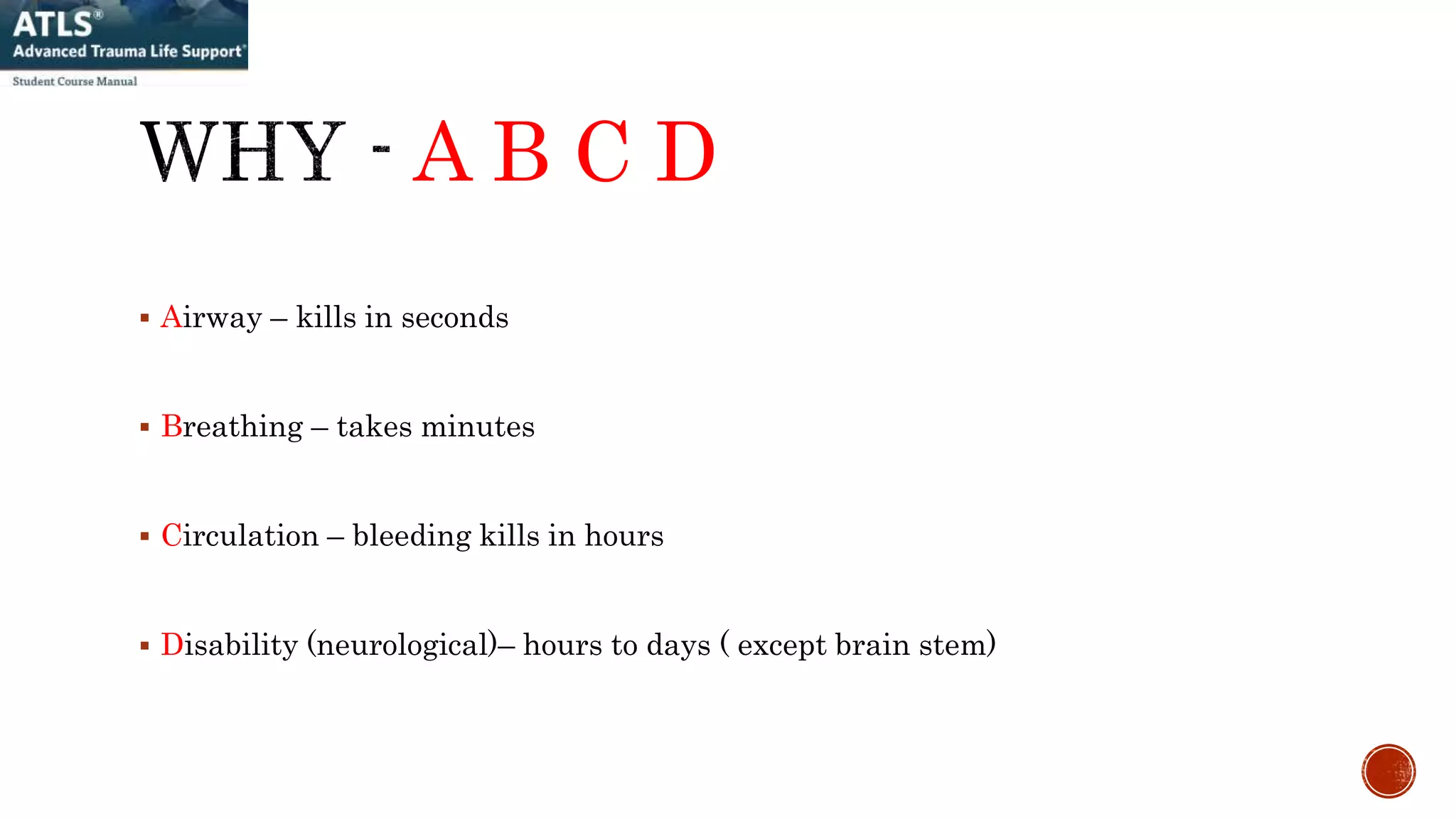
![Approach_to_the_trauma_patient[1].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/approachtothetraumapatient1-220906191256-c4d92395-thumbnail.jpg?width=640&height=640&fit=bounds)









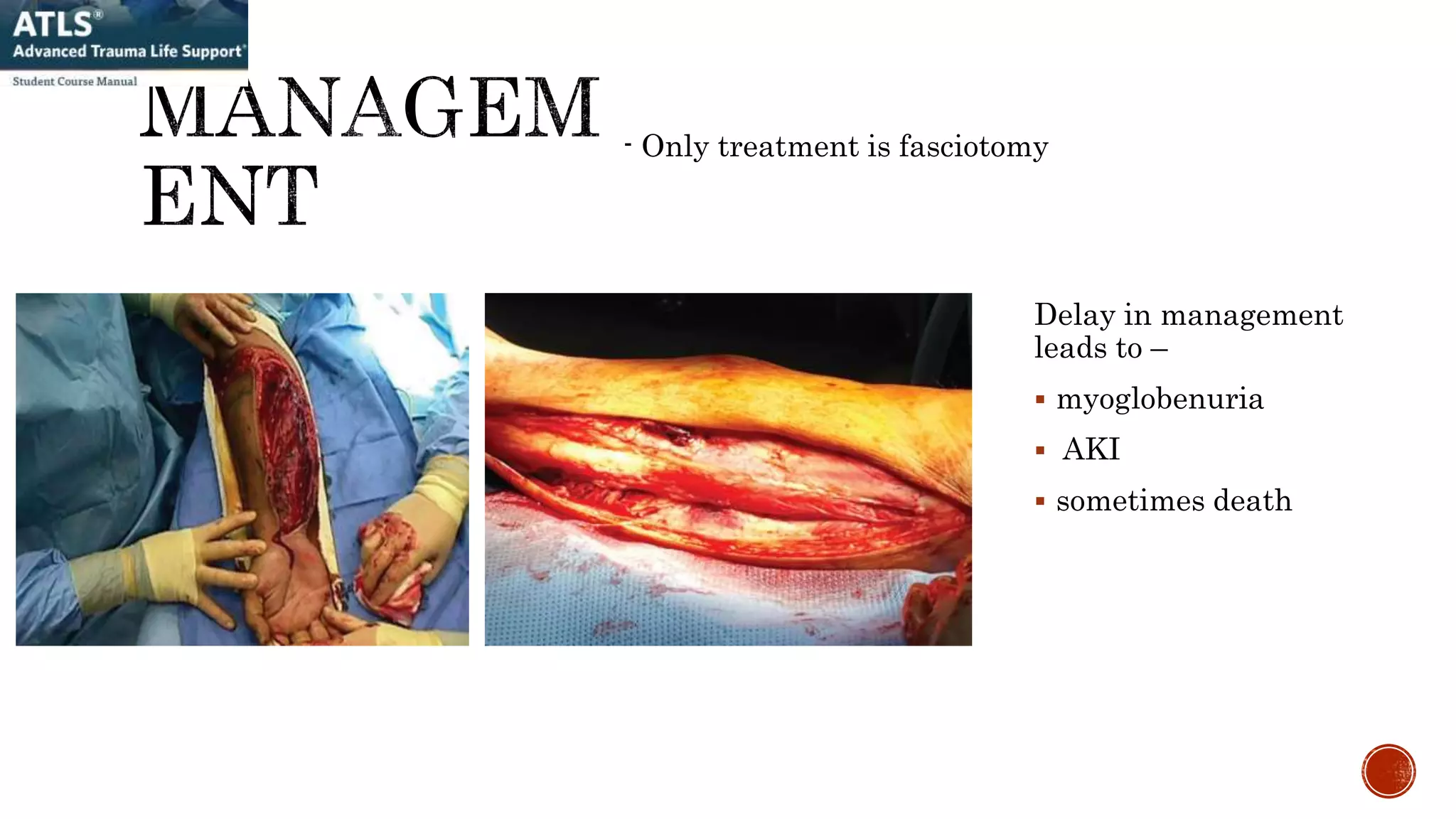
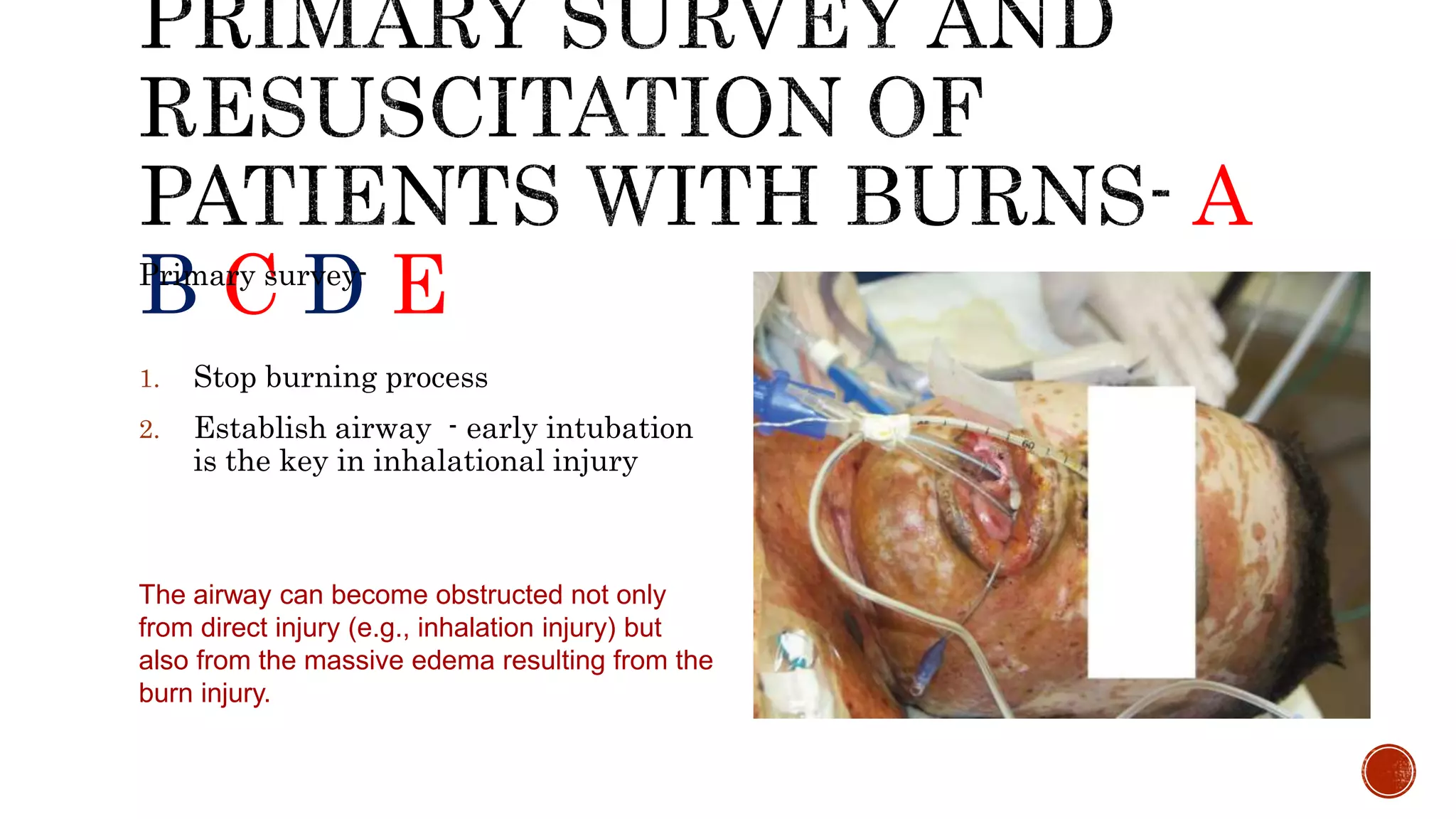
![Red_Trauma_Management_Presentation[1].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/redtraumamanagementpresentation1-250623235639-3b1285fd-thumbnail.jpg?width=640&height=640&fit=bounds)











































