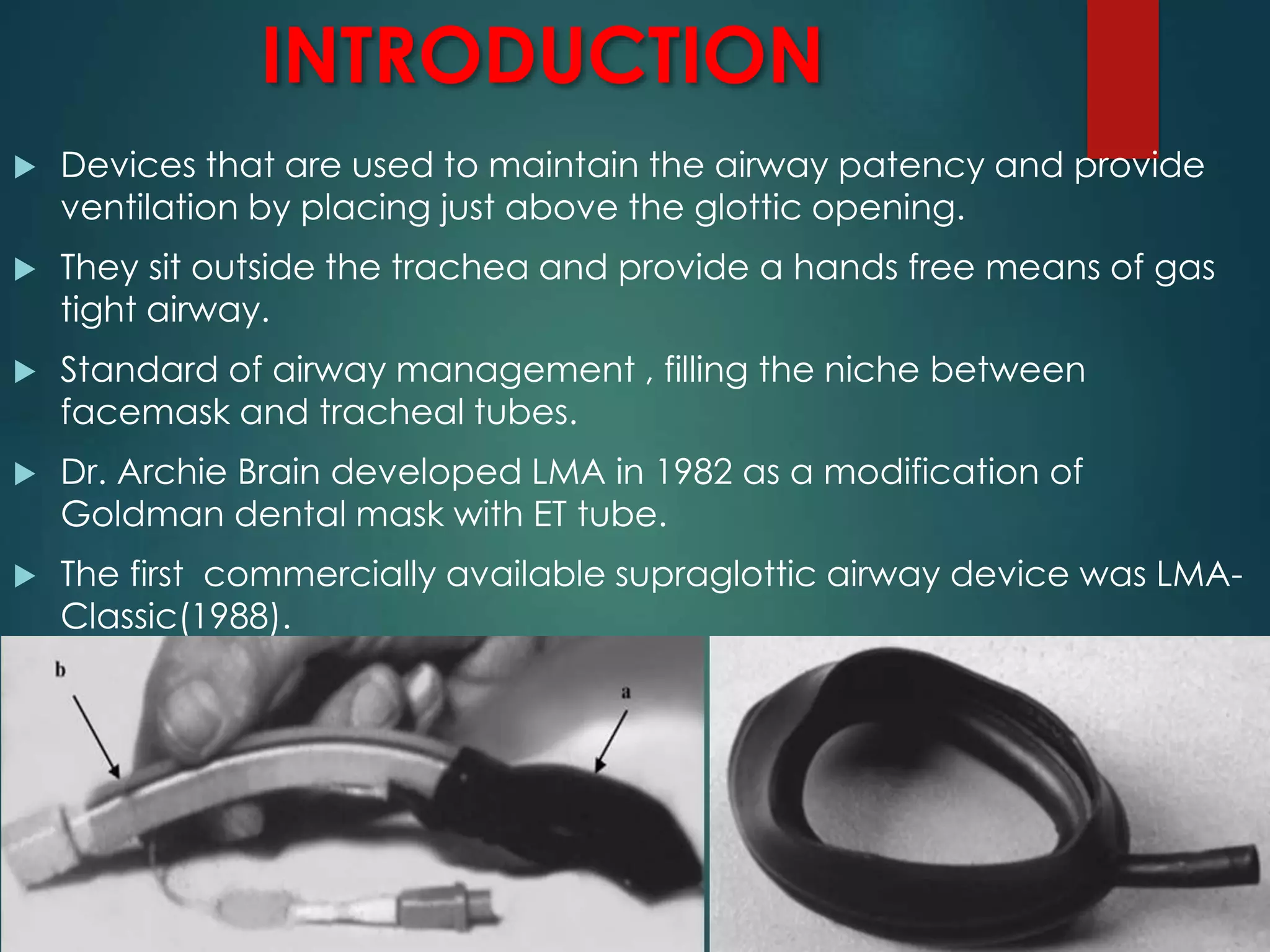
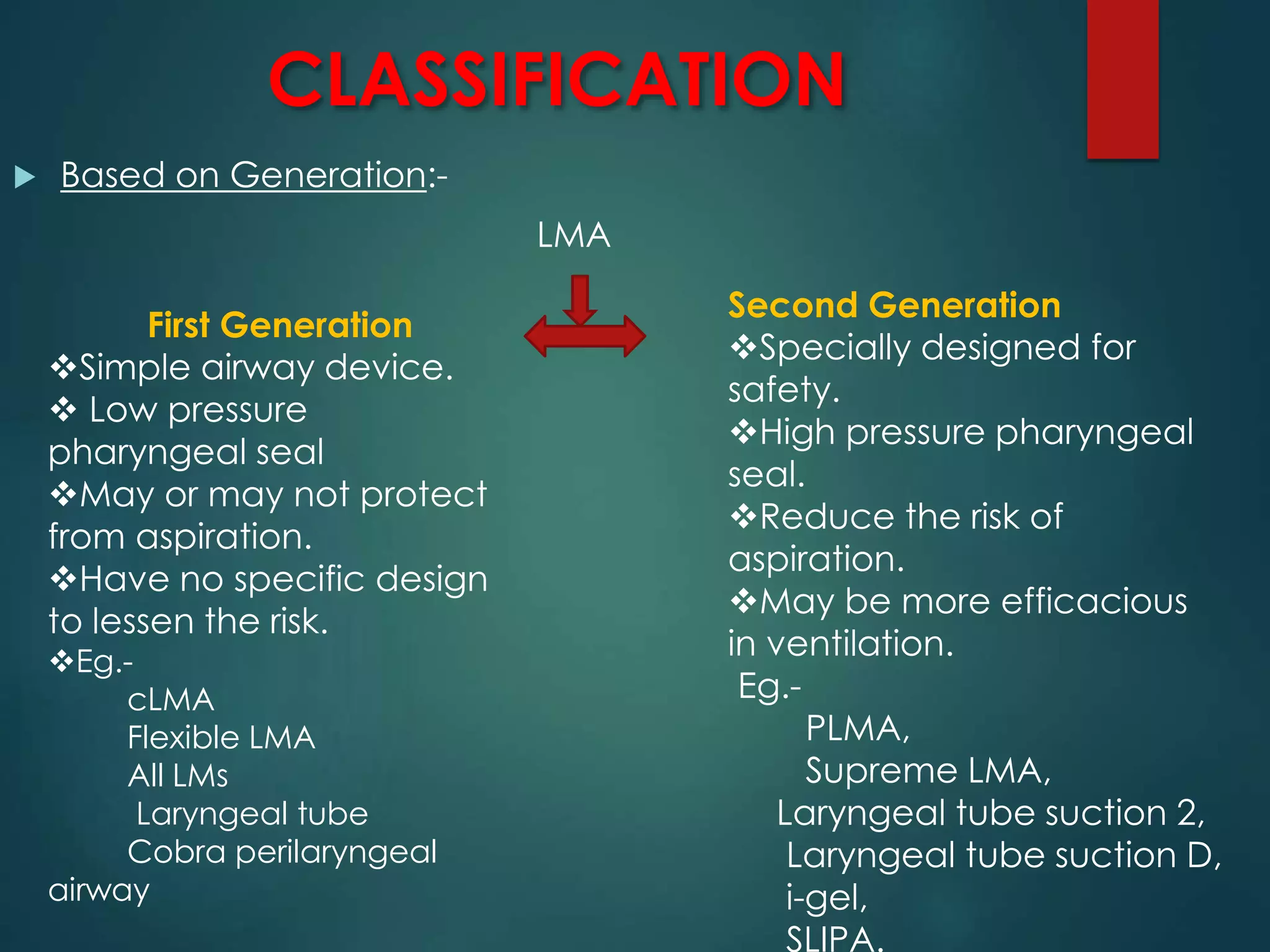
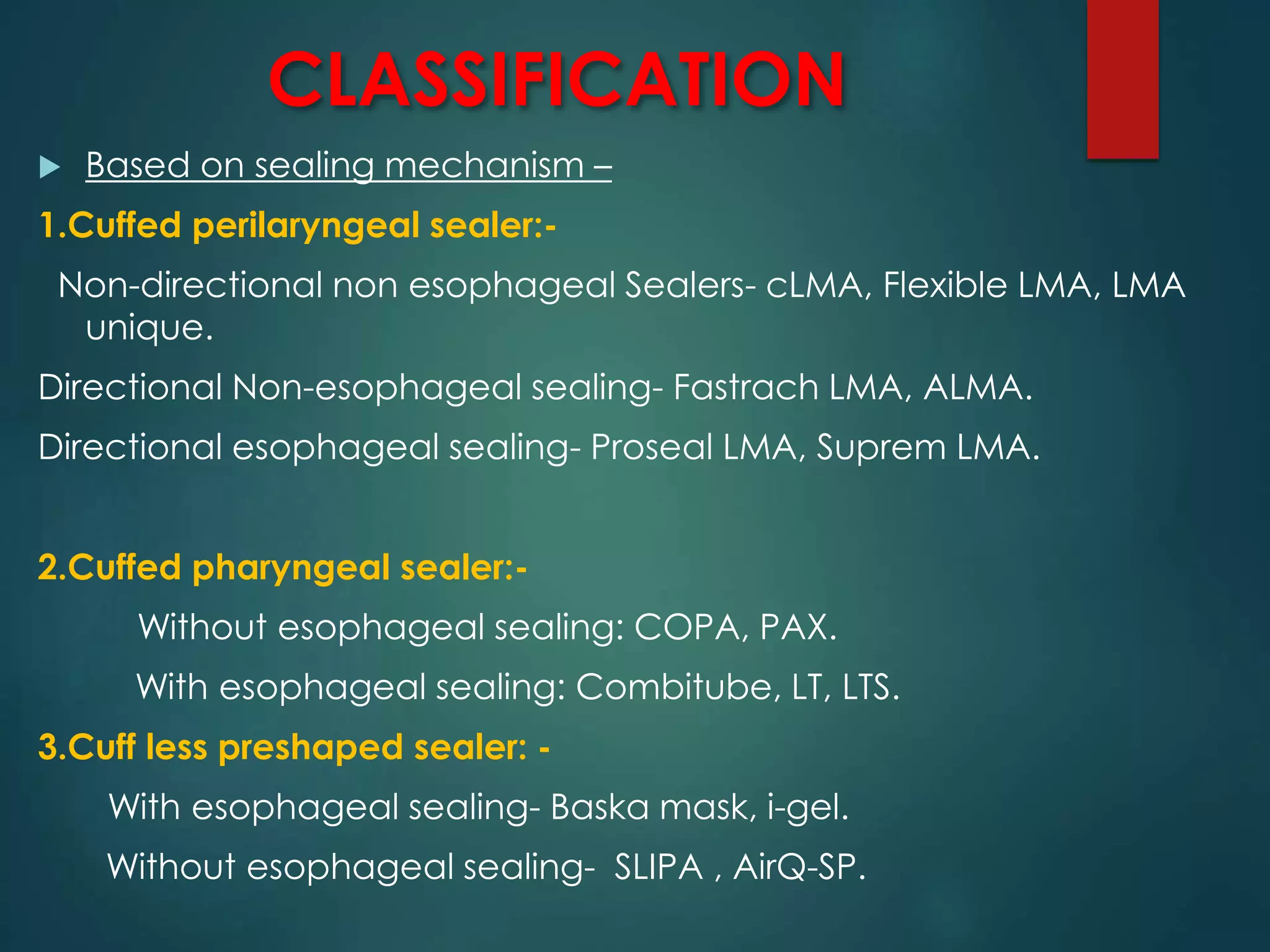
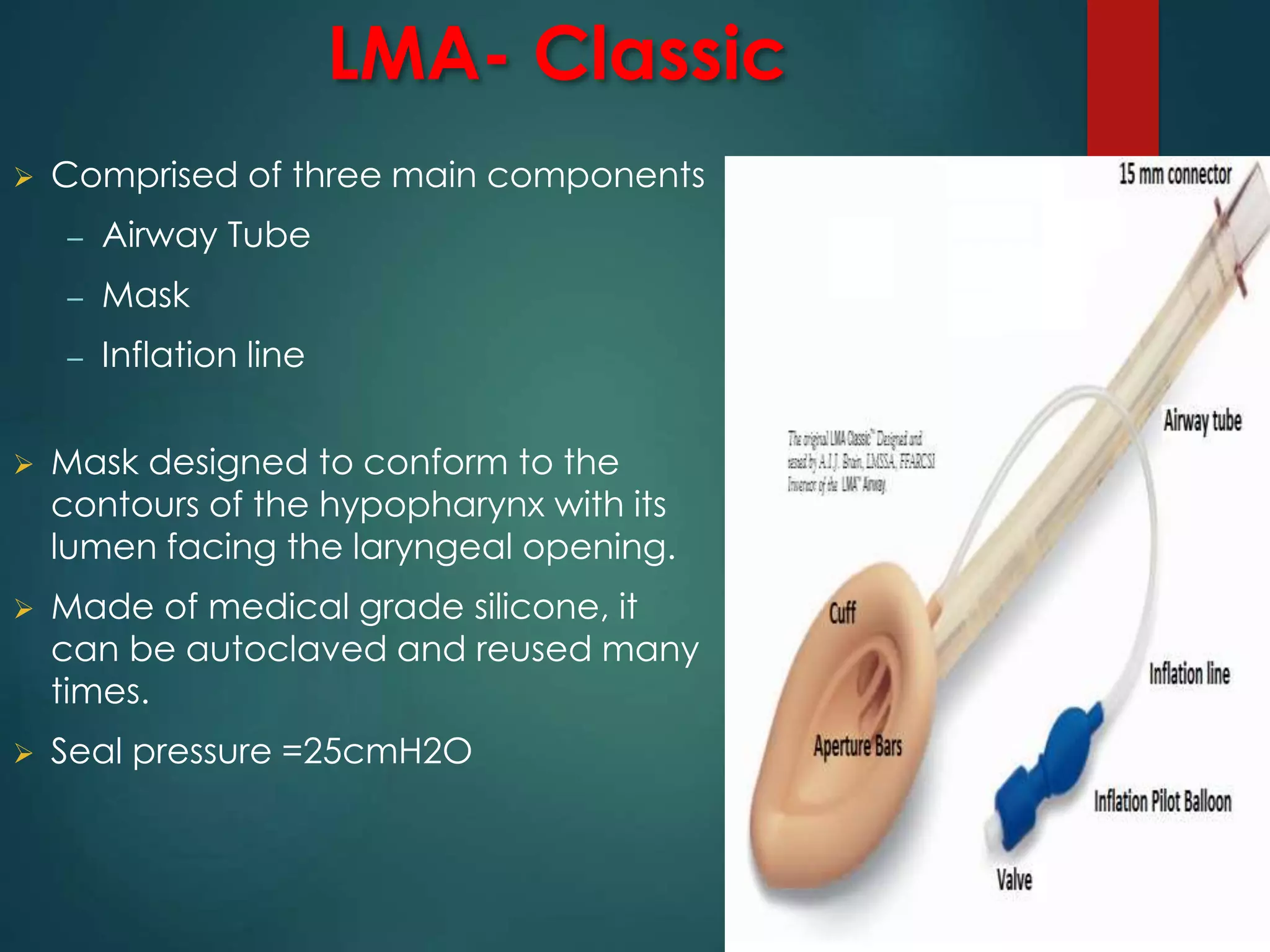
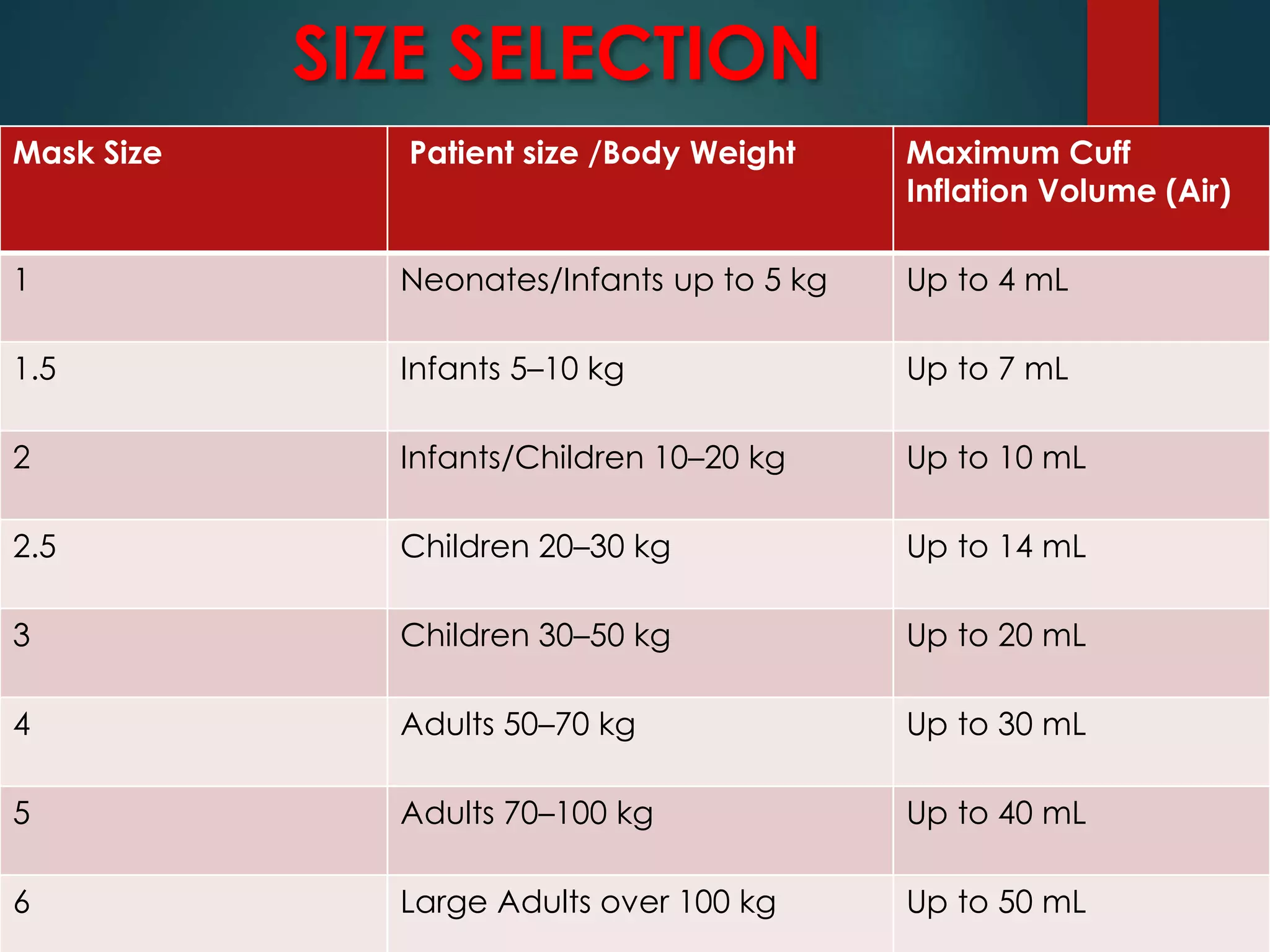
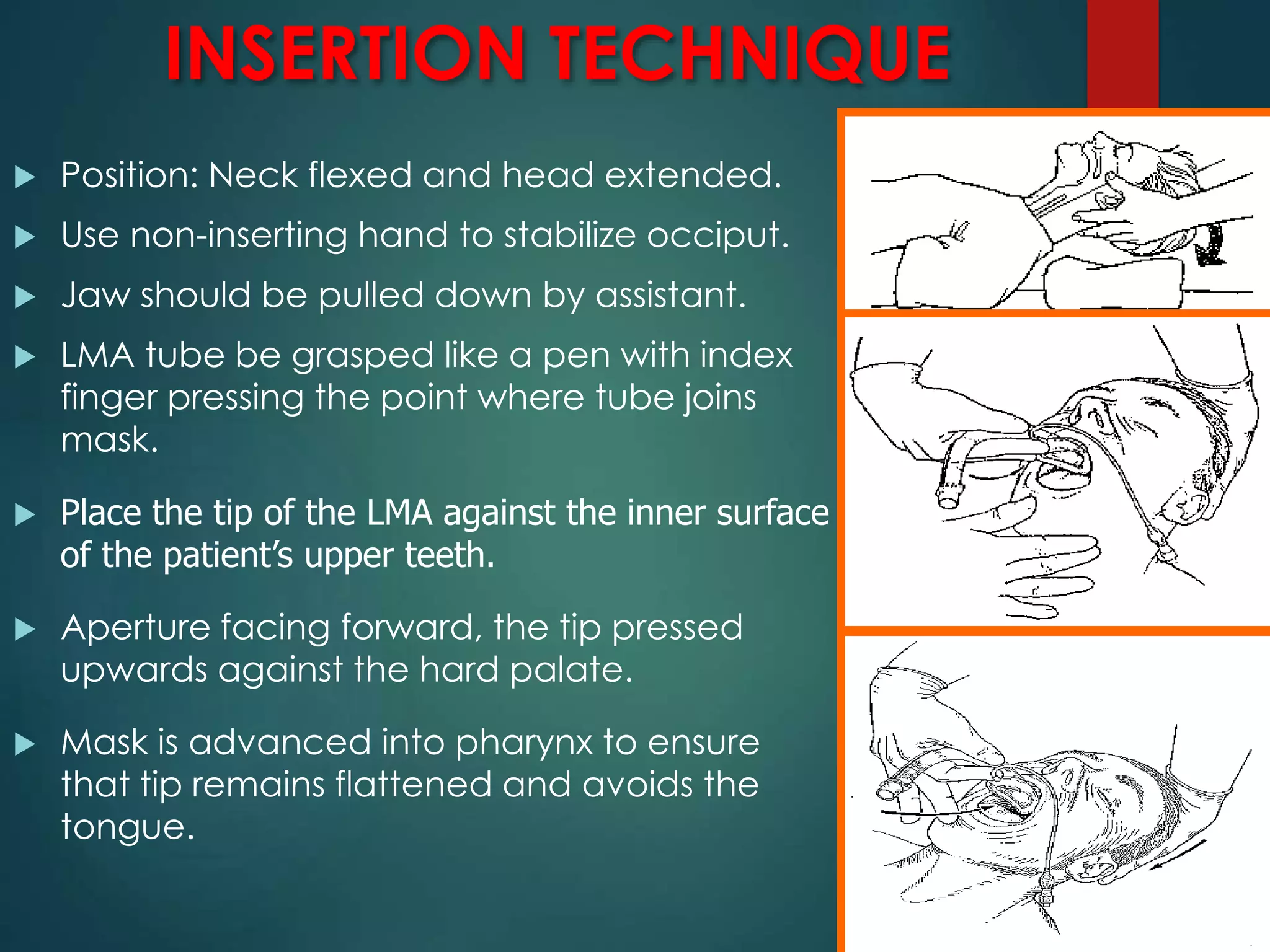
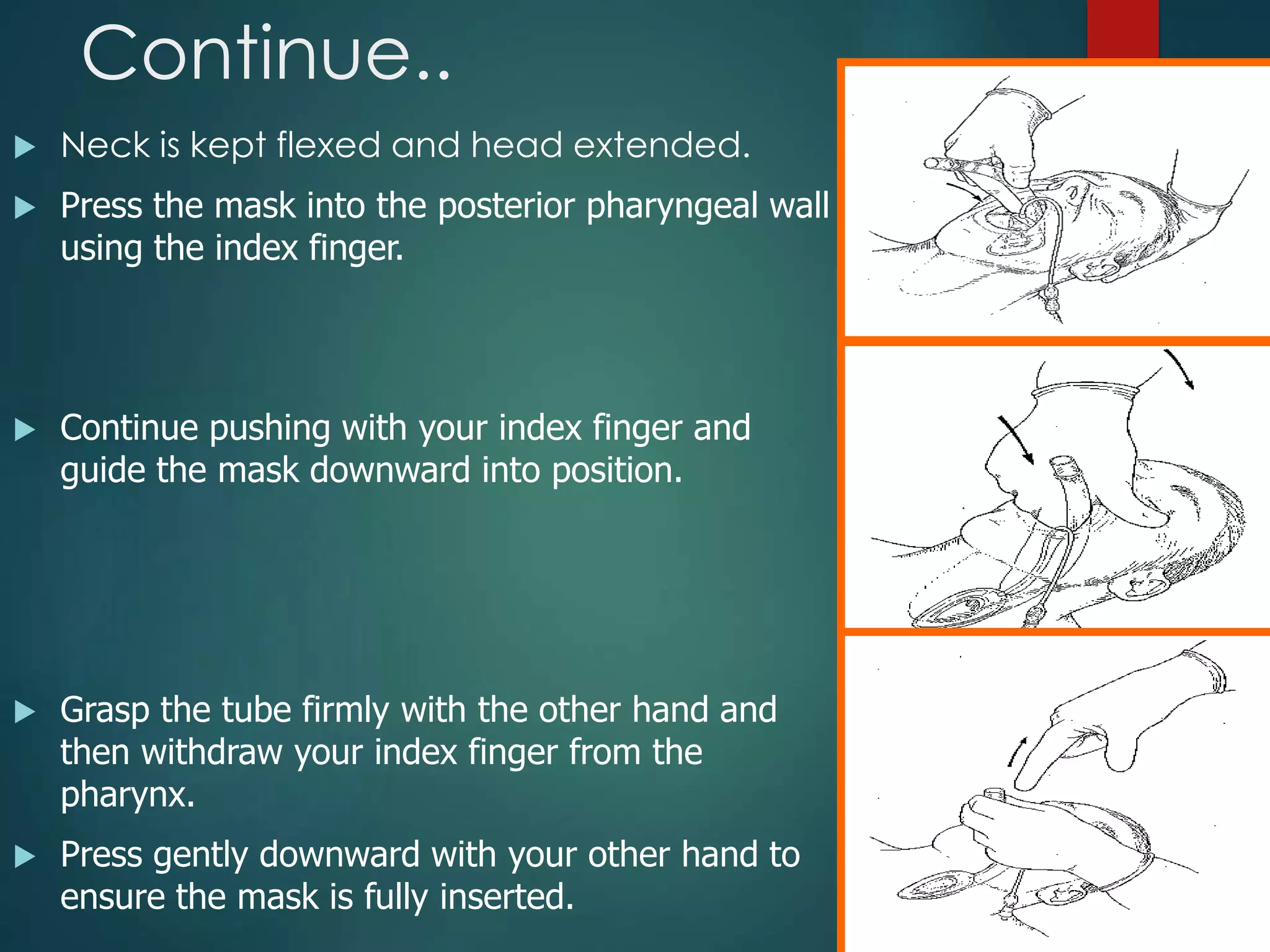
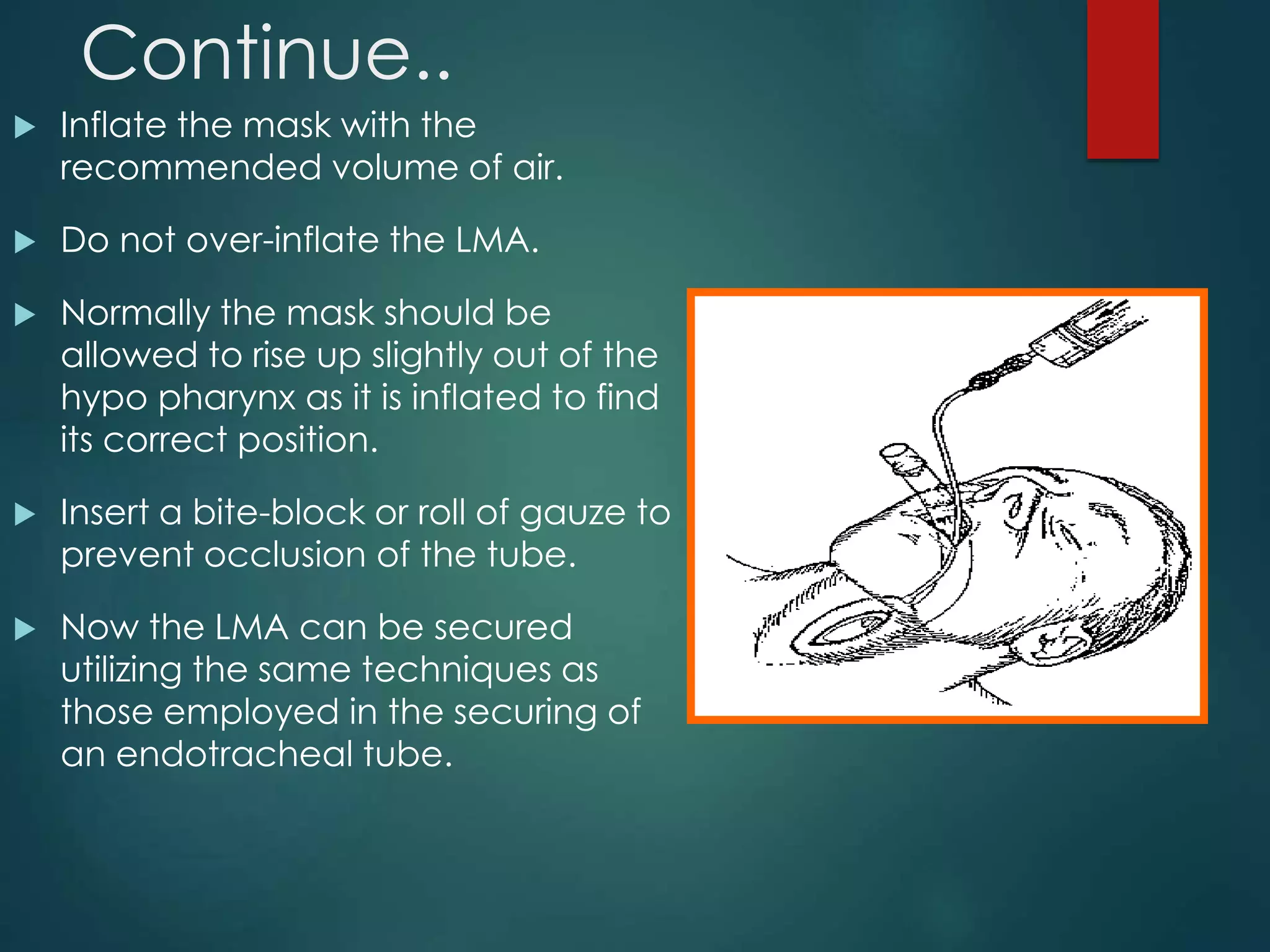
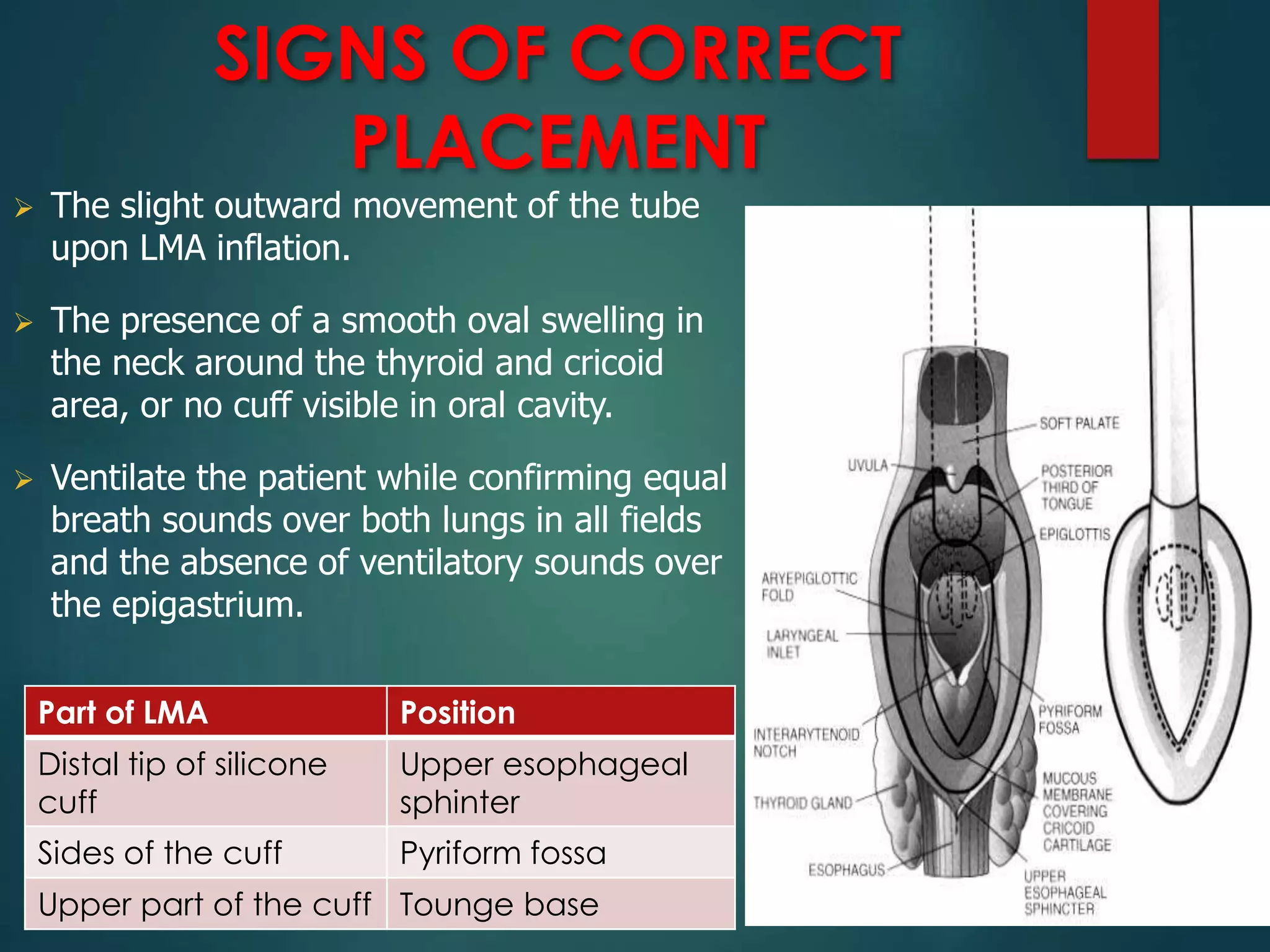
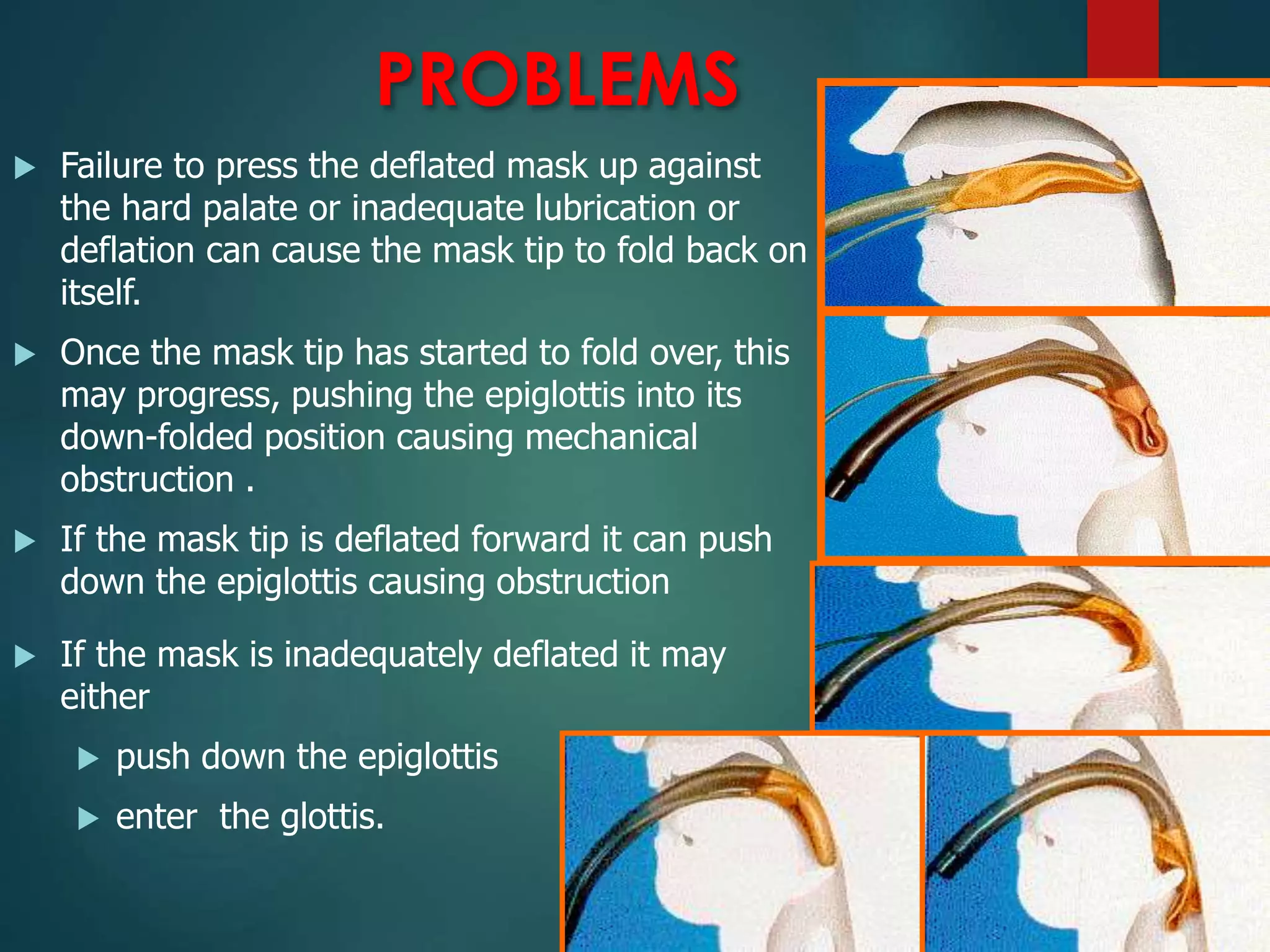
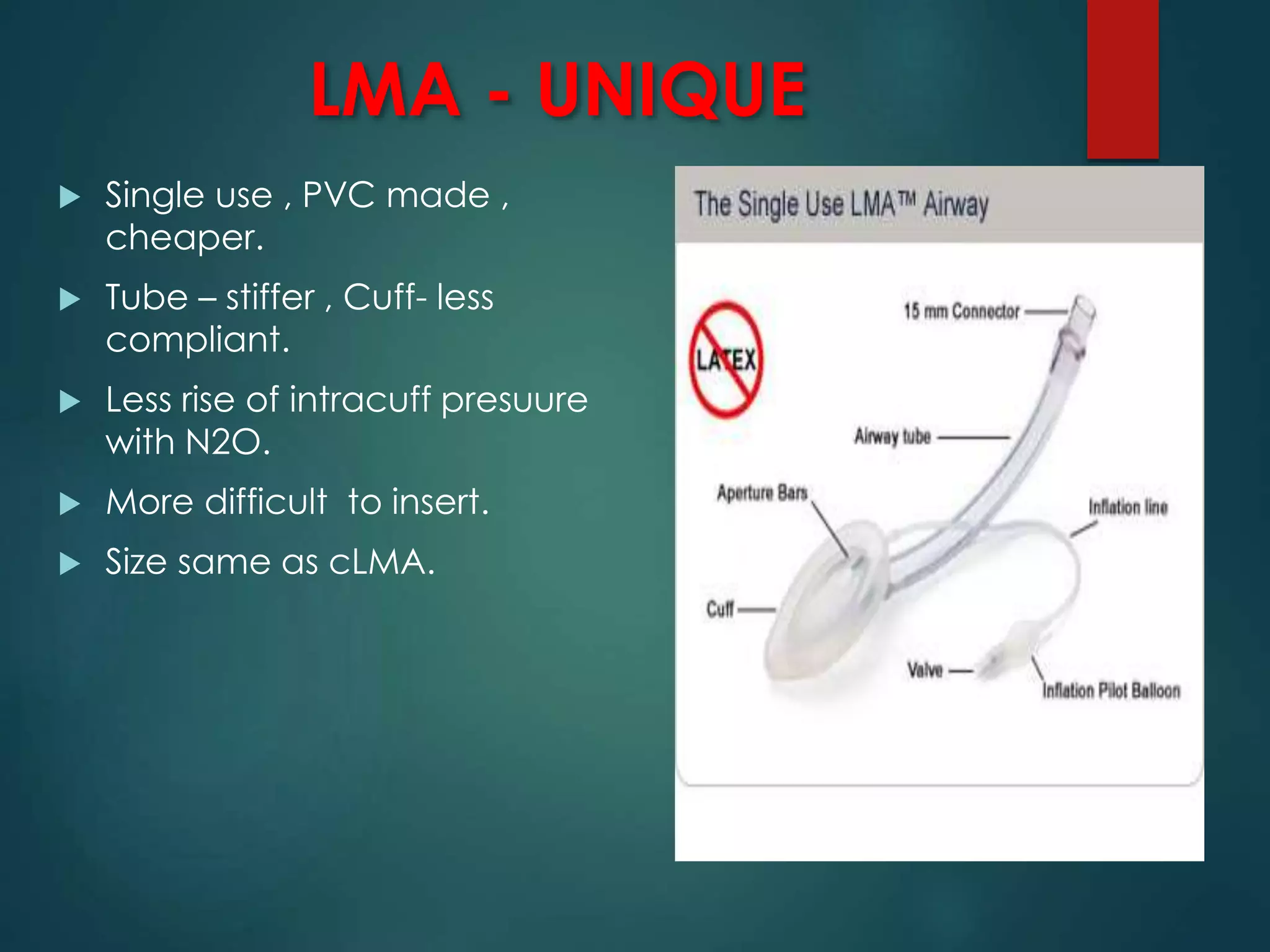
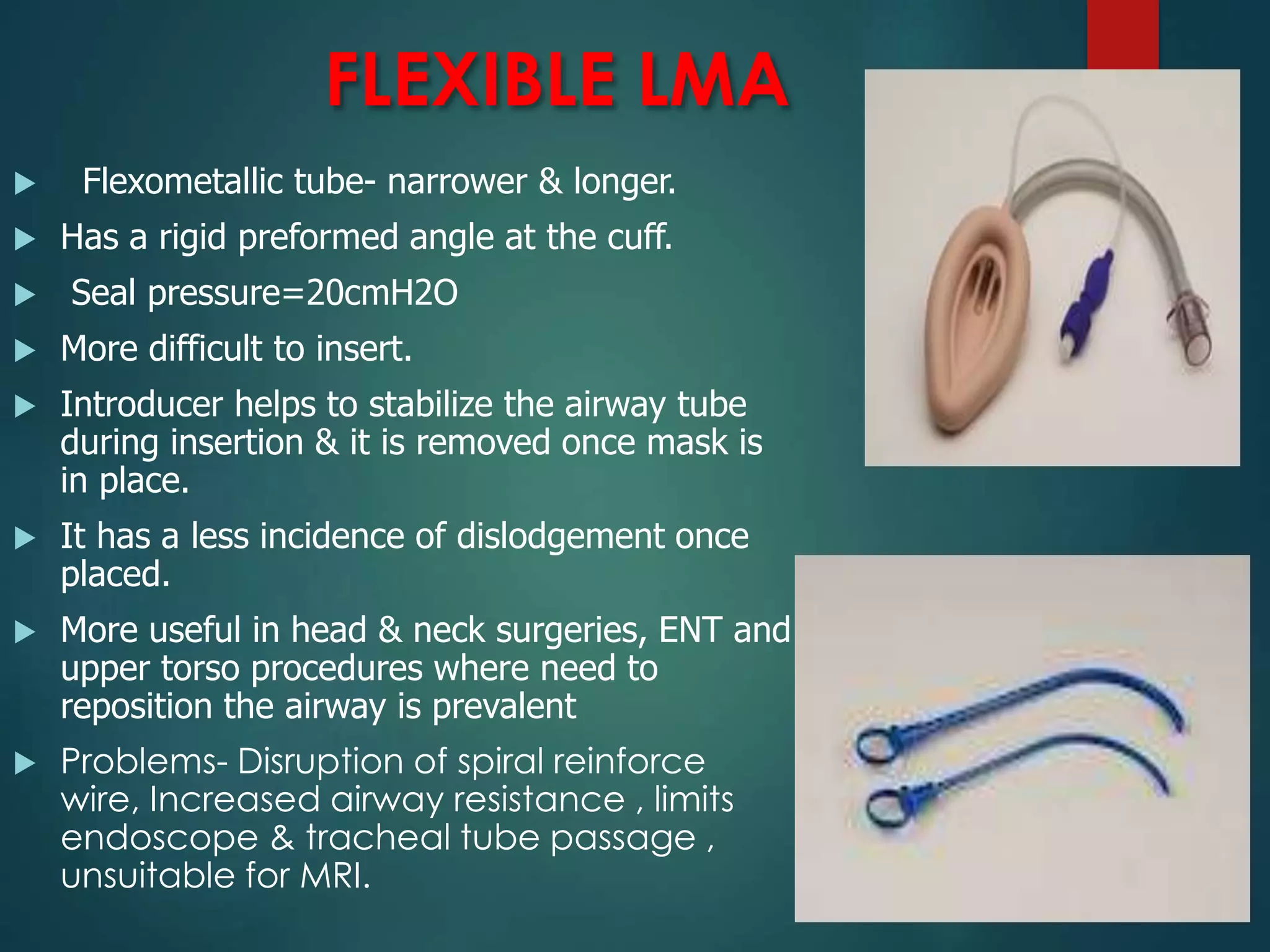
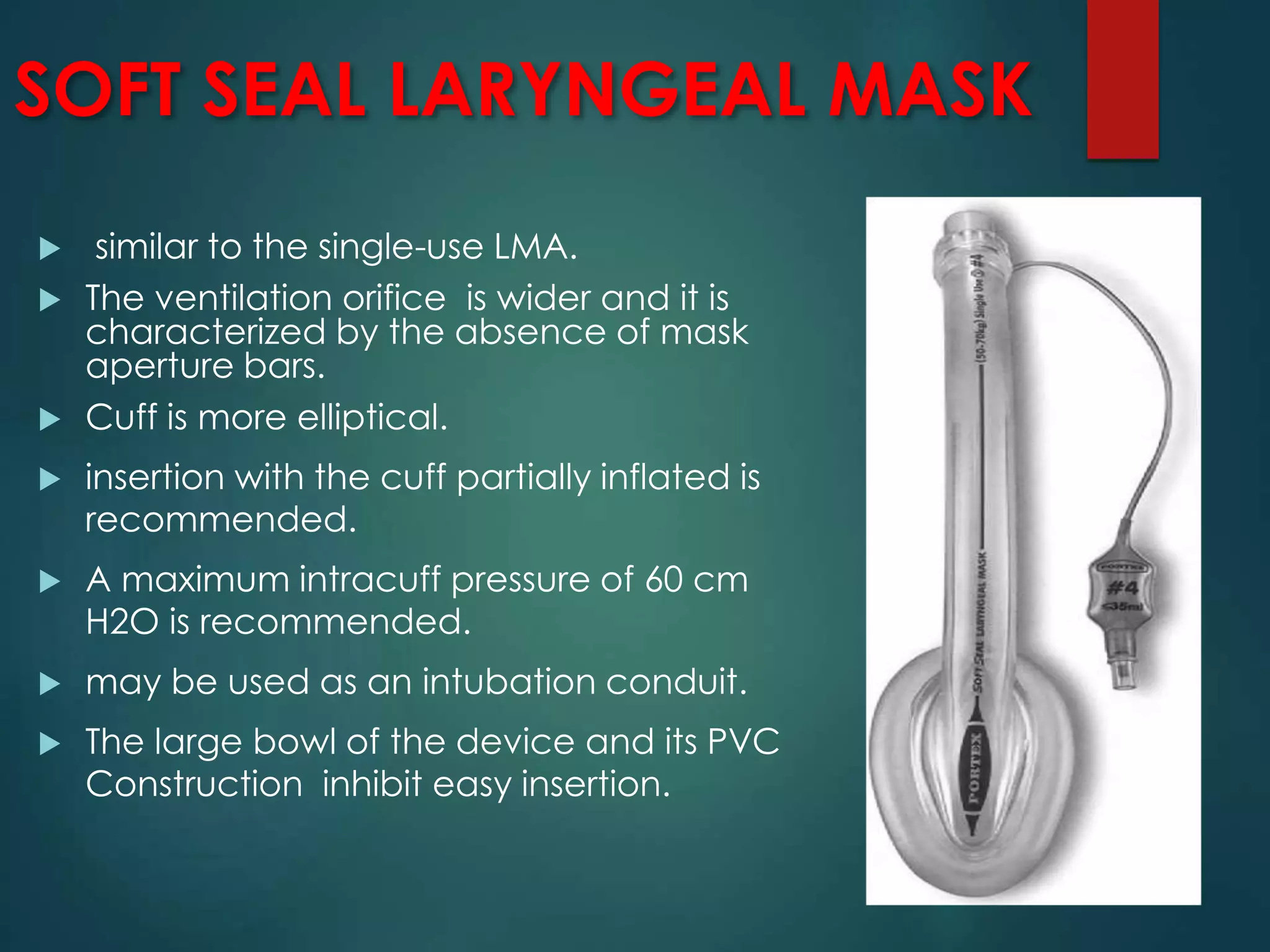
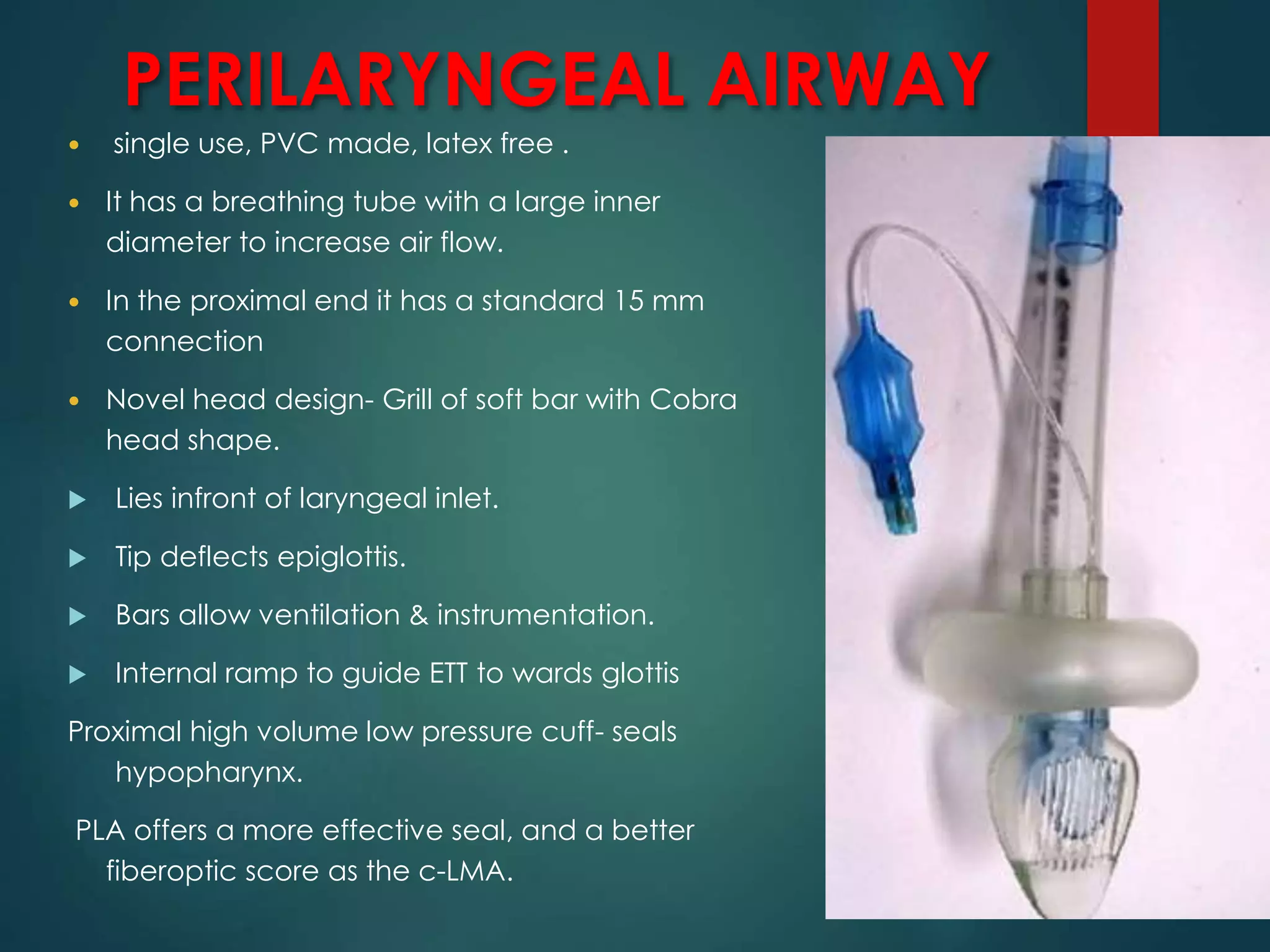
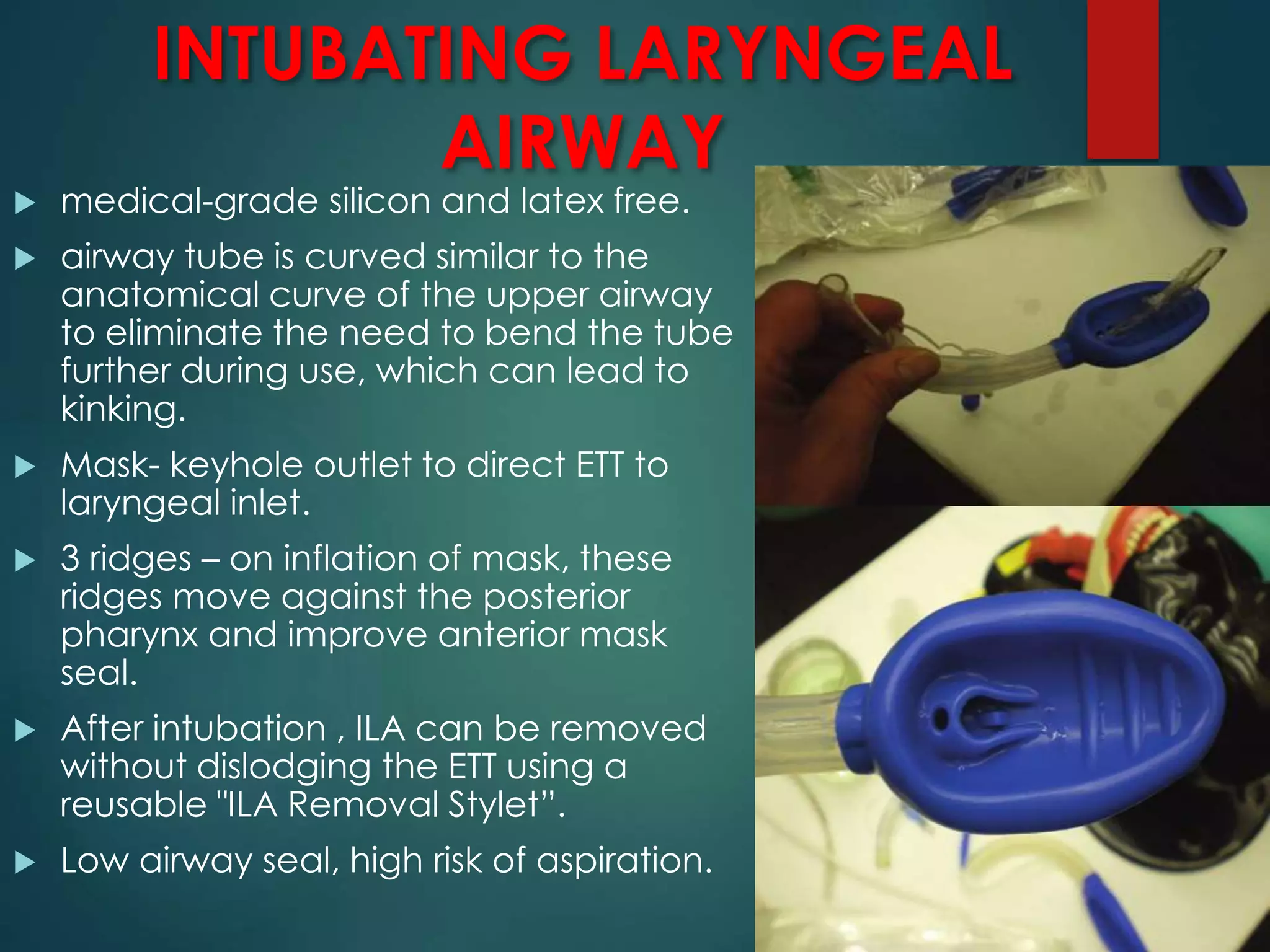
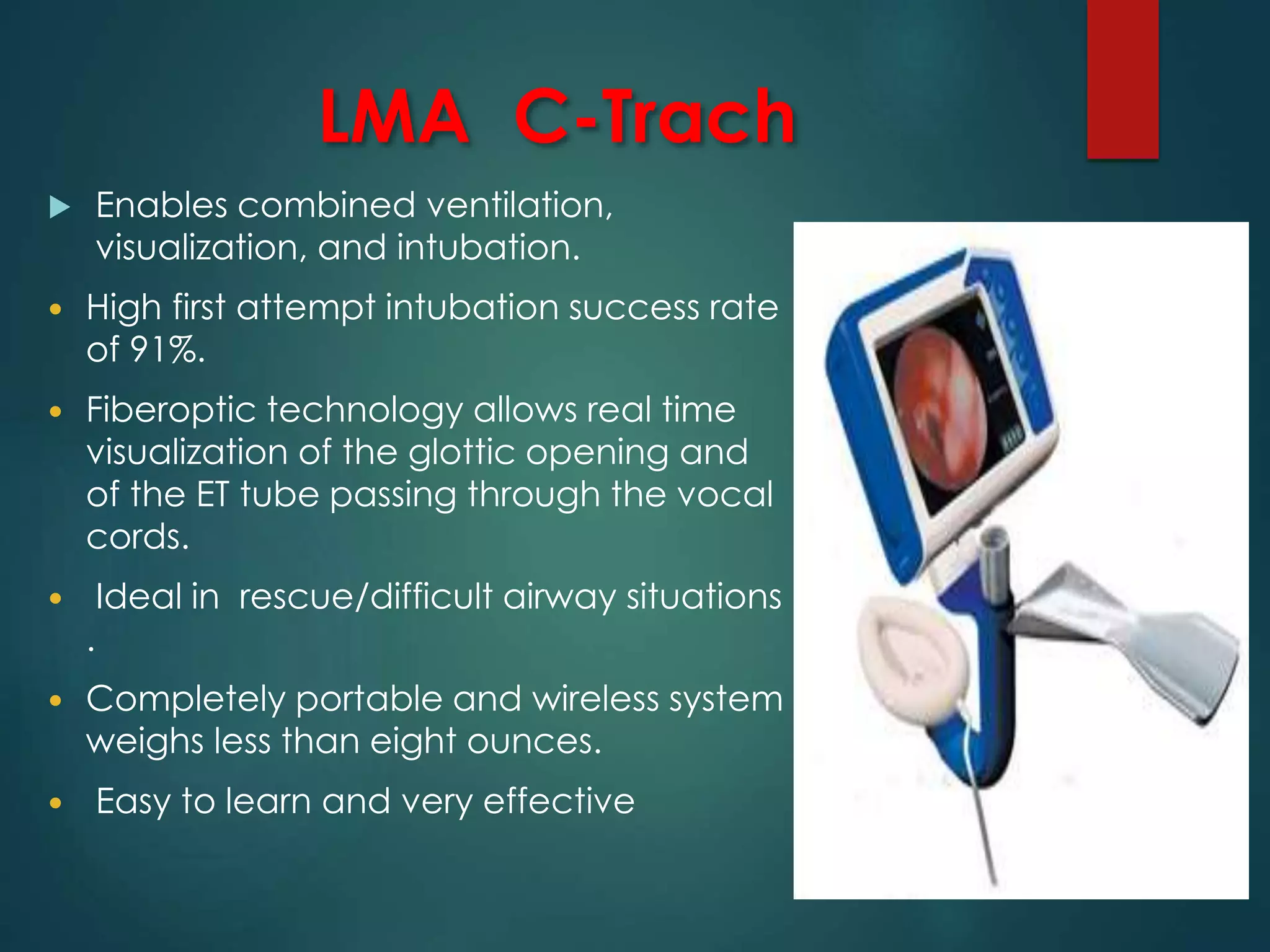
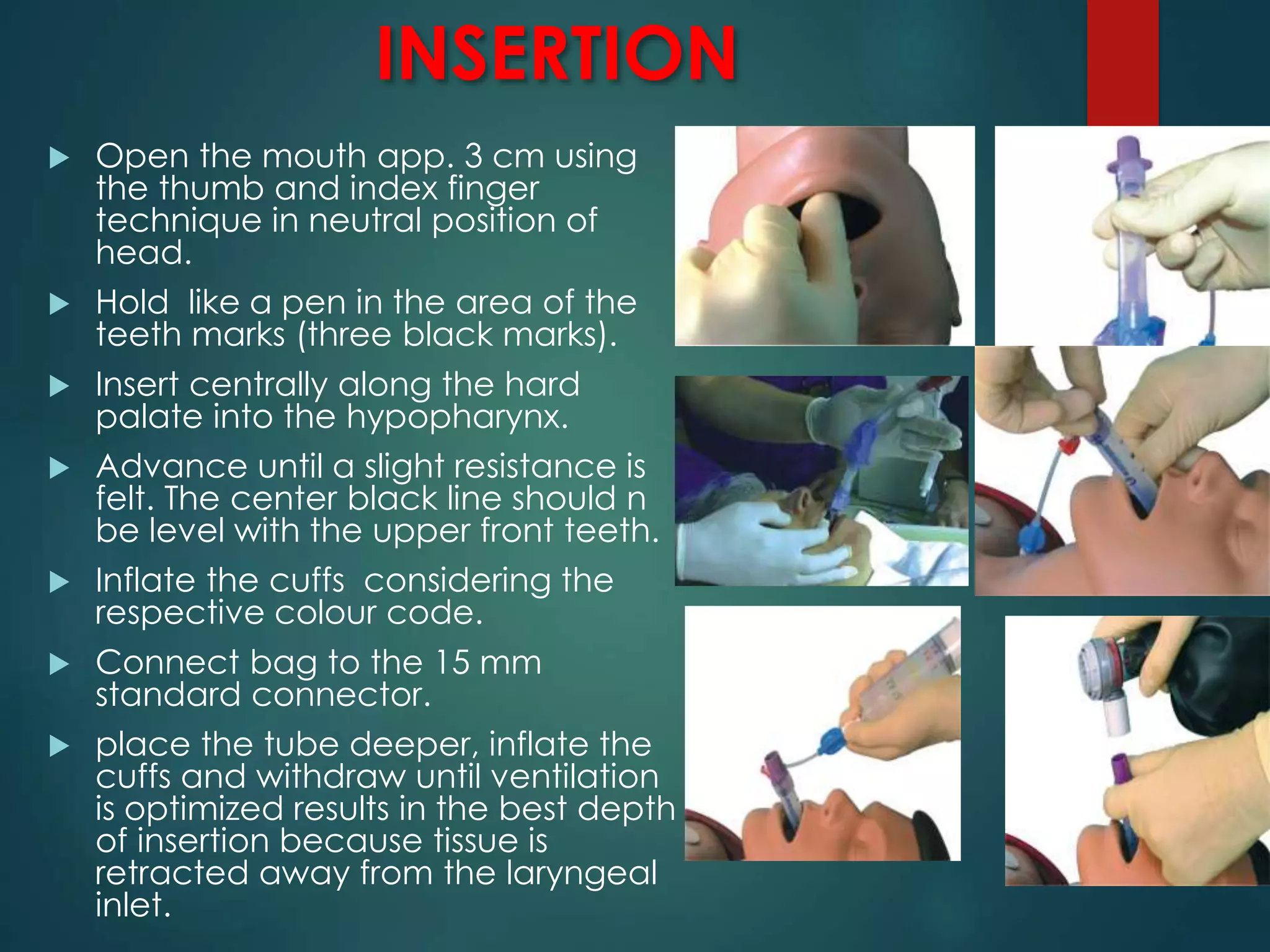
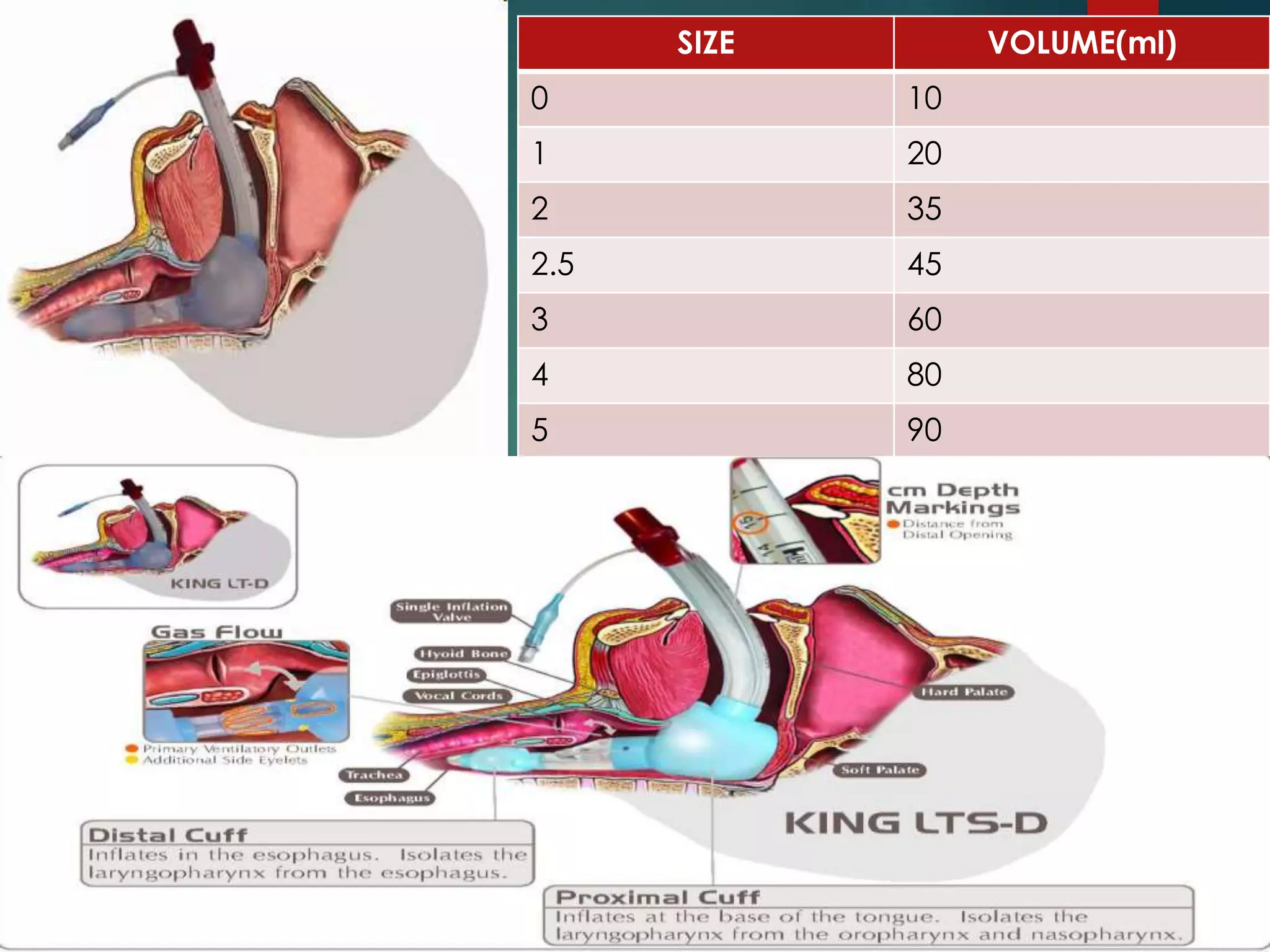
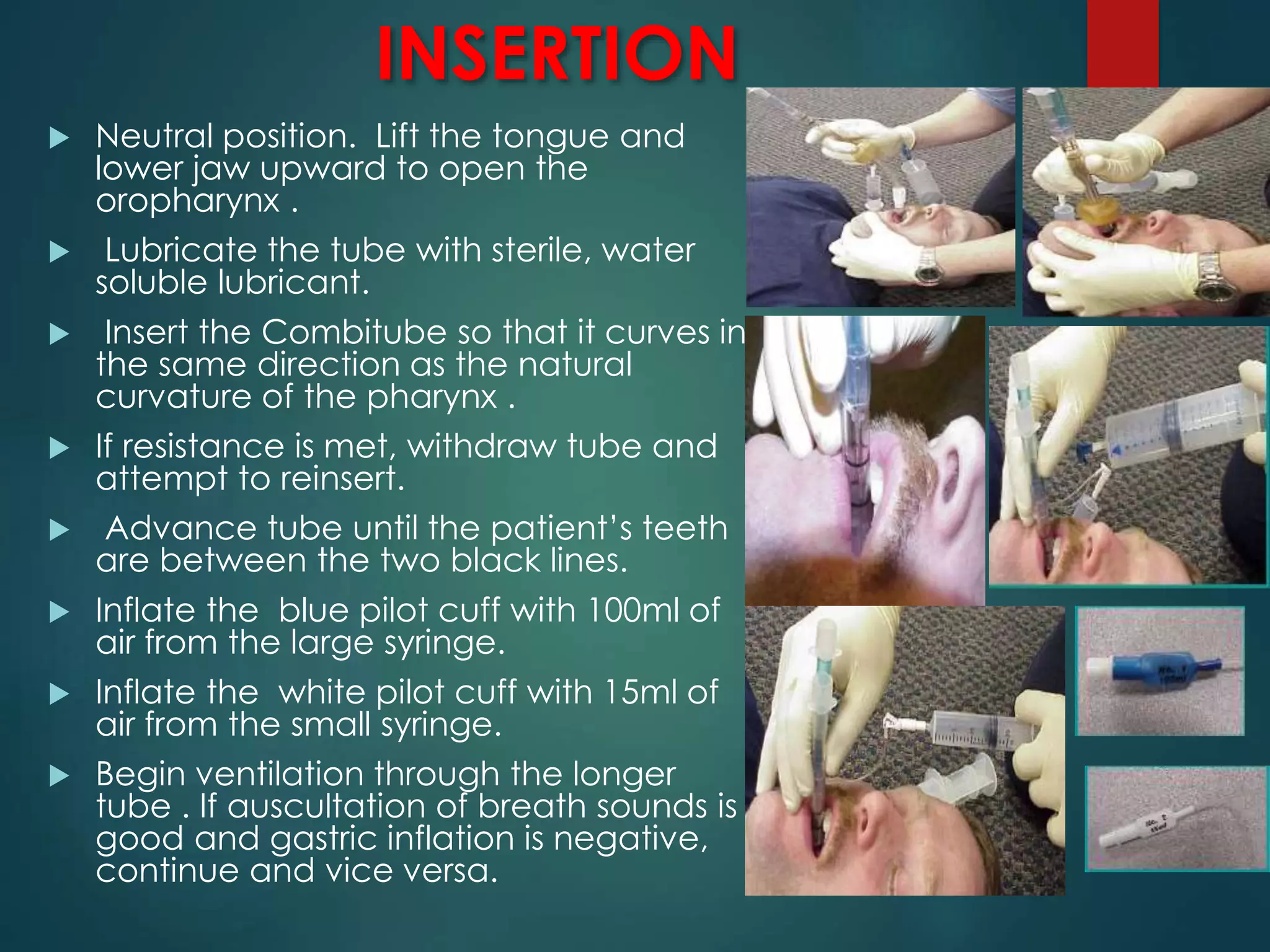
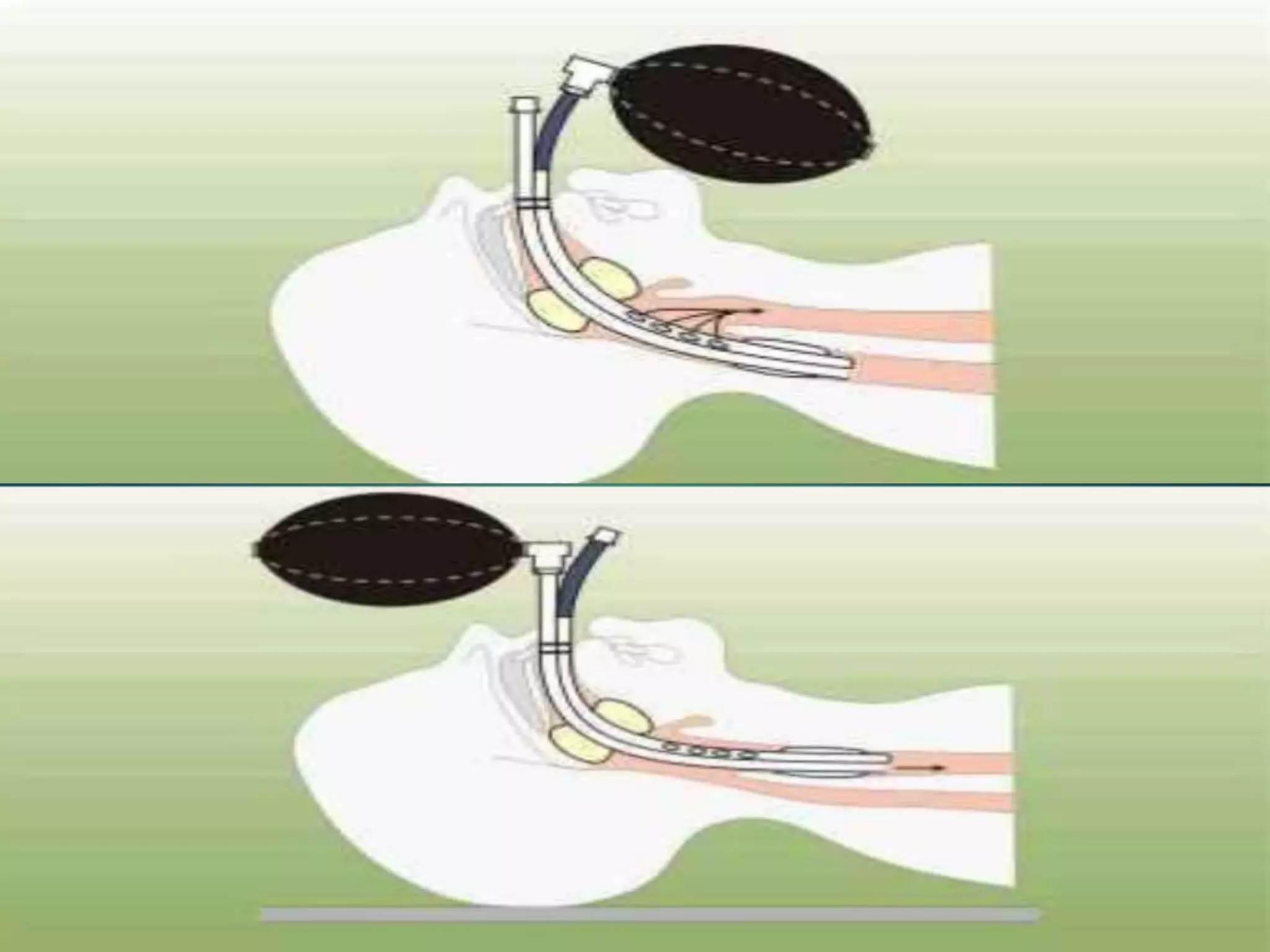
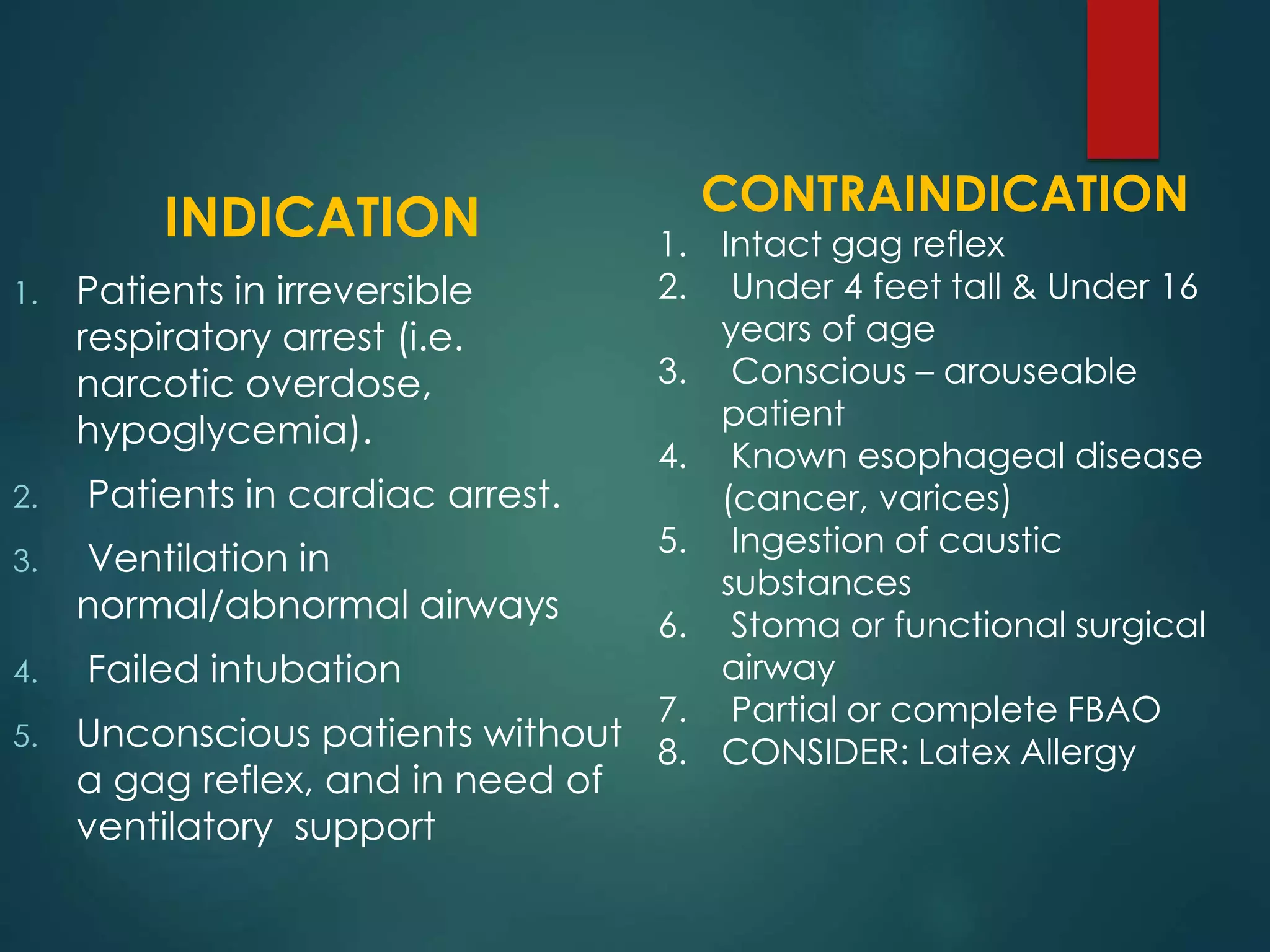
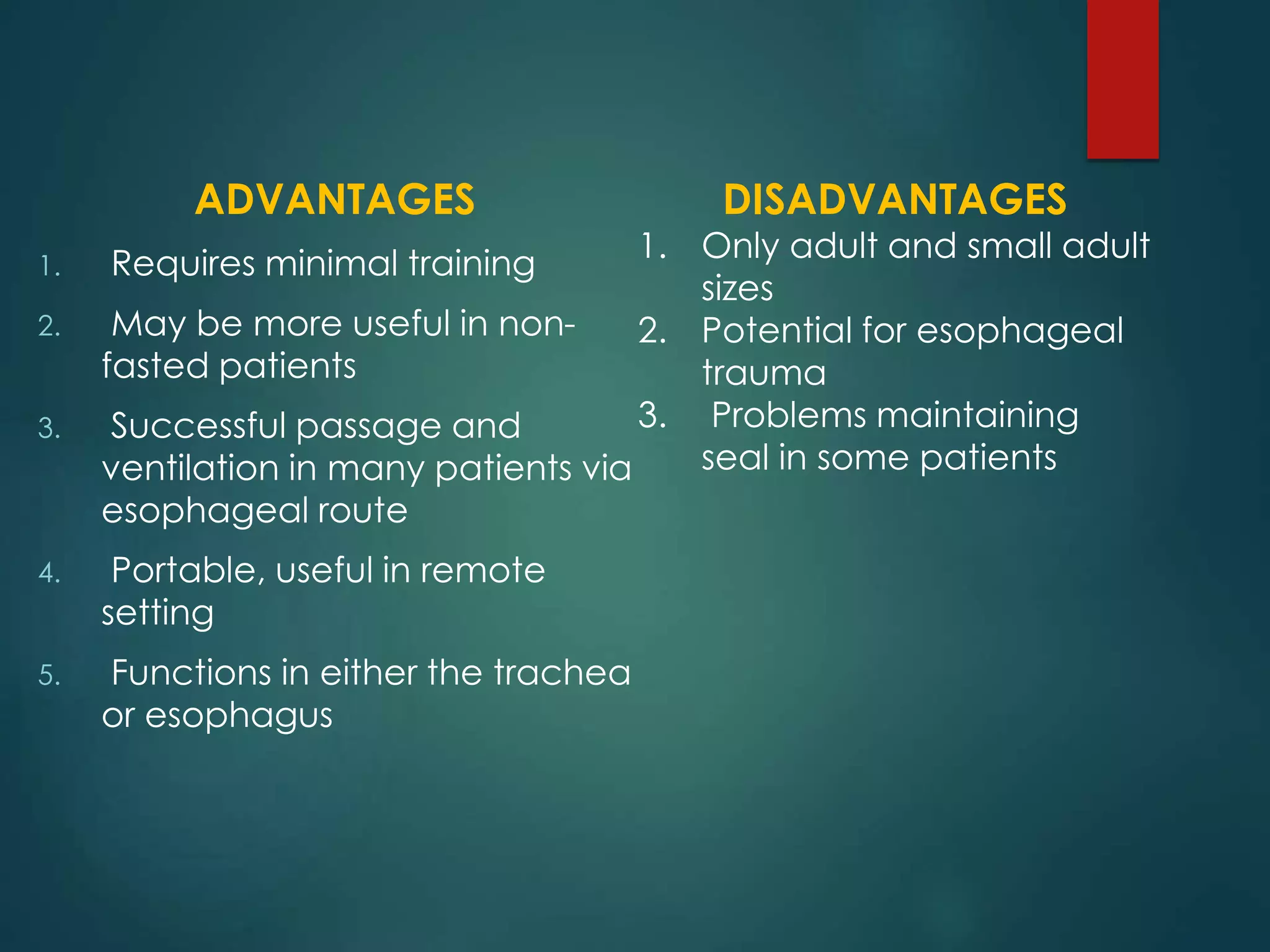
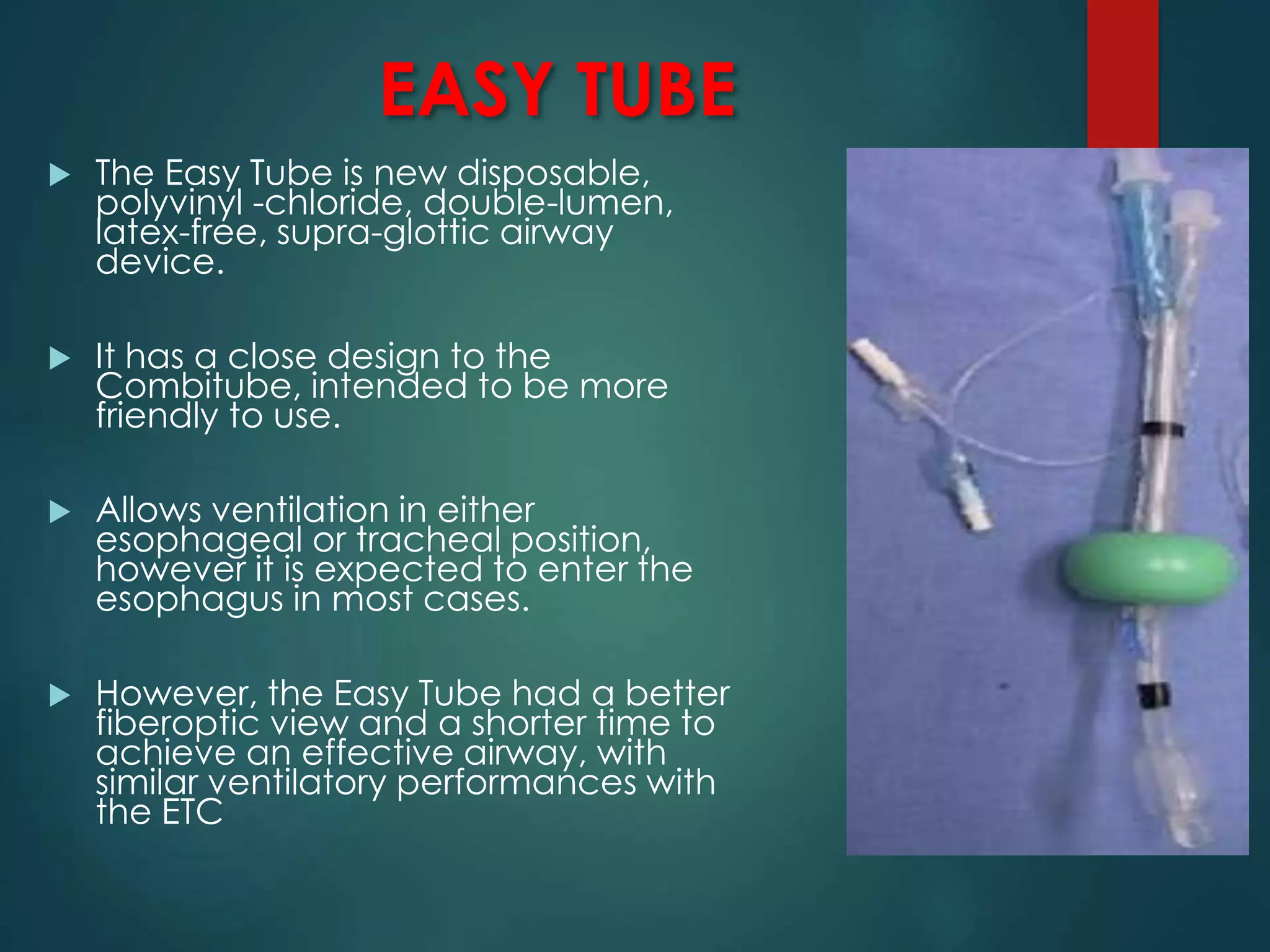
This document discusses supraglottic airway devices. It begins by introducing supraglottic airway devices and their purpose of maintaining airway patency above the glottic opening. It then classifies supraglottic devices based on generation, sealing mechanism, number of lumens, and discusses some common devices like the LMA Classic, Unique, Flexible, and Ambu Aura. Indications, contraindications, advantages, disadvantages, proper sizing, insertion technique and signs of correct placement are outlined. Potential problems and methods to reduce aspiration are also reviewed.