1) Supraglottic airways facilitate oxygenation and ventilation without endotracheal intubation. They are classified based on their sealing mechanism and evolution of design, with over 17 variants discussed.
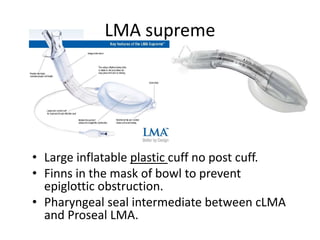
2) Key devices include the Classic LMA, Proseal LMA, i-Gel, Laryngeal Mask Airway, and Laryngeal Tube. Each was developed to address shortcomings of prior models, such as improved sealing pressures and drainage.
3) Supraglottic airways are recommended by Difficult Airway Society guidelines for use in both anticipated and unanticipated difficult airway scenarios, and have been used successfully in airway rescue cases when other methods fail