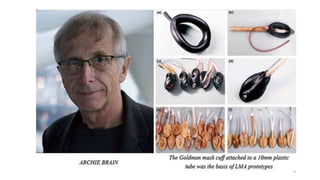
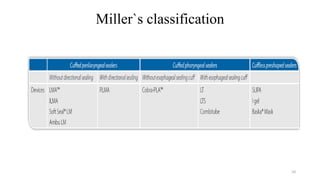
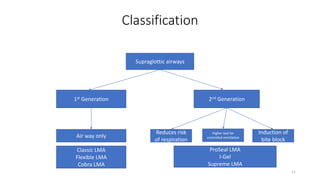
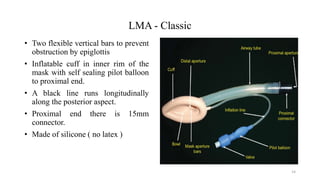
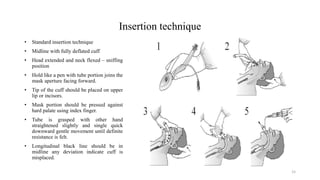
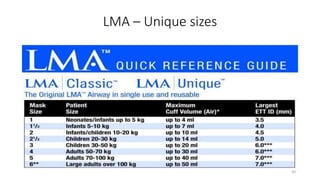
The document discusses supraglottic airway devices like the Laryngeal Mask Airway (LMA), describing the different types of LMAs including 1st generation devices like the Classic LMA and 2nd generation devices like the ProSeal LMA. It covers how to use LMAs, indicating them for elective procedures, difficult airways, and cardiopulmonary resuscitation. The document also addresses contraindications, complications, advantages and disadvantages of LMAs compared to other airway management options.


































































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)







