1. Staphyloccus aureus - Microbiology with references
Staphylococcus aureus
References :
Ananthnarayan and Panikers Textbook of Microbiology
Apurba Sankar Sastry and Sandhya Bhat - Essentials of Medical Microbiology-Jaypee Brothers Medical Publishers
Textbook of Microbiology – Dr. C.P. Baveja
Gram Positive Cocci(GPC)
• Gram-positive cocci are classified into two families Micrococcaceae
and Strepcococcaceae, differentiated by the catalase test.
• Micrococcaceae are catalase positive, gram-positive cocci arranged in
tetrads or clusters
• Where as Strepcococcaceae are catalase negative gram positive cocci,
arranged in pairs or chains.
5.
• Staphylococcus speciesare arranged in clusters, show fermentative
pattern in oxidative fermentative test
• Among Staphylococcus species, S. aureus is the most pathogenic; it
produces an enzyme coagulase which forms the basis of coagulase
test
• Whereas, other species do not produce coagulase and are called as
coagulase-negative Staphylococcus (CoNS).
6.
Family – Micrococeae
Genus– Staphylococcus
Classification
A. Based on pigment production
• Staphylococcus aureus – Golden yellow
• Staphylococcus albus – White colonies
• Staphylococcus citrus – Lemon yellow colonies
B. Based on pathogenicity
• Pathogenic – Staphylococcus aureus
• Non-Pathogenic – S. epidermidis, S. albus
C. Based on Coagulase production
• Coagulase positive – S.aureus
• Coagulase negative – S.epidermidis, S. saprophyticus
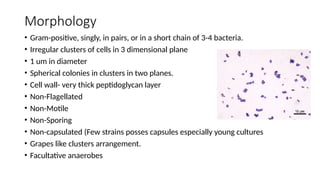
Morphology
• Gram-positive, singly,in pairs, or in a short chain of 3-4 bacteria.
• Irregular clusters of cells in 3 dimensional plane
• 1 um in diameter
• Spherical colonies in clusters in two planes.
• Cell wall- very thick peptidoglycan layer
• Non-Flagellated
• Non-Motile
• Non-Sporing
• Non-capsulated (Few strains posses capsules especially young cultures
• Grapes like clusters arrangement.
• Facultative anaerobes
10.
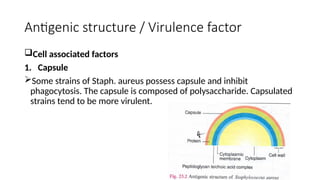
Antigenic structure /Virulence factor
Cell associated factors
1. Capsule
Some strains of Staph. aureus possess capsule and inhibit
phagocytosis. The capsule is composed of polysaccharide. Capsulated
strains tend to be more virulent.
11.
2. Peptidoglycan
Peptidoglycanis a polysaccharide polymer that provides rigidity to the cell
wall. It activates complement and evokes production of inflammatory
cytokines.
3. Teichoic Acid
It is a major antigenic determinant of all strains of Staph. aureus. It is the
group specific ribitol teichoic acid of the cell wall. It facilitates adhesion of
the cocci to the host cell surface and protects them from complement
medicated opsonisation. It is associated with the peptidoglycan in an
insoluble form. It is absent in Staph. epidermidis. The latter contains glycerol
teichoic acid.
12.
4. Protein A
Itis a cell wall component of most strains of Staph. aureus (especially
Cowan I strain). It is chemotactic antiphagoocytic, anticomplementary
and elicits platelet injury. Protein A has ability to bind the Fc portion of
immunoglobulin G (IgG). Binding IgG in this manner can block
phagocytosis. Cowan I strains coated with any IgG antiserum will be
agglutinated if mixed with its corresponding antigen. This procedure is
known as Coagglutination. i.e. role in Co-agglutination test.
13.
Extracellular factors (Cytolytictoxins)
1. Toxins
membrane active substances
Four types of haemolysins are produced by staphylococci
i. Alpha haemolysin
• most important protein inactivated at 70°C but reactivates at 100°C
• lyses rabbit erythrocytes, but is less active against sheep & human red cells
• It is also leucocidal, Cytotoxic, dermonecrotic (on intradermal inoculatios in rabbits), neurotoxic and lethal
• Toxic to macrophages, Lysosomes, muscle tissues & renal cortex.
ii. Beta hemolysin
• Sphingomyelinase C, hemolytic for Sheep cells, but not human or rabbit erythrocytes.
• lysis is initiated at 37°c but it is evident only on cold temperature so, is named as hot-cold phenomenon.
• Produced both aerobically as well as anaerobically.
iii. Gamma lysin
• Acts on human, sheep and rabbit erythrocytes
iv. Delta lysin
• lytic to human, sheep and rabbit red blood cells.
14.
2. P-V Toxin/ Leucocidin
Panton–Valentine
3. Epidermolytic / Exfoliative Toxin
Cause scalded skin syndrome
Toxic epidermal necrolysis (TEN)
Ritter’s syndrome
4. Enterotoxins
Responsible for food poisoning
Incubation period of 1-6 hrs
(Can be because of S.aureus from milk, bakery product or poultry)
Can be because of B.cereus from Chinese food)
Act on vagus nerve and act on vomiting centre
5. TSST (Toxicshock syndrome toxin)
It is Enterotoxin F
It is superantigen
Risk Factor or Classical history : Vaginal tampons
Clinical features : Rash, Fever, low BP
And if not treated then multi organ failure
Diagnosis : Latex agglutination test , RIA, ELISA
17.
Extracellular factors (Cytolytictoxins)
1. Enzymes
i. Catalase
ii. Free Coagulase
iii. Thermonuclease (Heat stable)
iv. Phosphatase
v. DNAase
vi. Lipases
vii. Hyaluronite
viii. Nuclease
ix. Staphylokinase (fibriolysin)
x. Protease
18.
Growth requirements
• Aerobesand facultative anaerobes
• Temperature range 10-42°C
• Optimum Temperature for growth = 37°C (35°C – 37°C)
• Optimum pH for growth = 7.5 (7.4 – 7.6)
• Grow on ordinary media
19.
Cultural characteristics
Media used
1.Non-selective Media
• Nutrient agar
• Blood agar
• Mac Conkey agar
2. Selective media
• SALT-Milk agar (8-10% NaCl)
• Lundlam’s Medium
20.
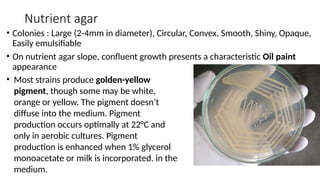
Nutrient agar
• Colonies: Large (2-4mm in diameter), Circular, Convex, Smooth, Shiny, Opaque,
Easily emulsifiable
• On nutrient agar slope, confluent growth presents a characteristic Oil paint
appearance
• Most strains produce golden-yellow
pigment, though some may be white,
orange or yellow. The pigment doesn’t
diffuse into the medium. Pigment
production occurs optimally at 22°C and
only in aerobic cultures. Pigment
production is enhanced when 1% glycerol
monoacetate or milk is incorporated. in the
medium.
21.
Note
• Golden yellowdue to production of pigment known as
staphyloxanthin (belongs to beta carotene group)
• Require 22°C , aerobic condition
• Non-diffusible pigment
22.
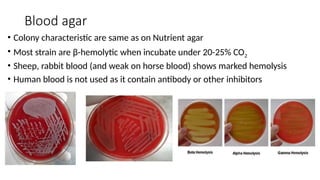
Blood agar
• Colonycharacteristic are same as on Nutrient agar
• Most strain are β-hemolytic when incubate under 20-25% CO2
• Sheep, rabbit blood (and weak on horse blood) shows marked hemolysis
• Human blood is not used as it contain antibody or other inhibitors
23.
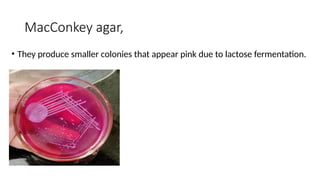
MacConkey agar,
• Theyproduce smaller colonies that appear pink due to lactose fermentation.
24.
• Liquid media
Thegrowth appears as uniform turbidity.
• Selective Media
Needed for isolating from specimen such as Feces
8-10% NaCl may be added to nutrient agar, Salt agar or Milk agar (Salt-milk
agar)
Mannitol salt agar
Lithium chloride & Tellurite agar
Ludlam’s medium
Polymyxin
25.
Biochemical properties
• Catalasepositive, Oxidase negative
• Coagulase positive: the presence of free and /or bound coagulase
• OF (oxidative-fermentative)test – fermentative
• Indole negative, Gas negative, Hydrogen sulfide negative
• Methyl red positive, VP positive
• Nitrate reduction positive (Nitrate to nitrite)
• Gelatin hydrolysis positive
• Citrate positive, Urease positive
• PYR negative
• DNA-ase test positive
• Phosphatase positive
• Phage typing
26.
Resistance
• more resistantamong non-sporing bacteria
• They survive in dried pus for 2-3 months.
• Most Staphylococci are killed at 62°C for 30 minute
• But hour some may require 80°C for one hour
• Most strains grow in presence of 10% NaCl
• Staphylococci are resistant to 1% phenol for 15 minutes while
mercury per chloride (1%) solution kills in 10 minutes.
• Staphylococci and resistant to lysozyme sensitive to lysostaphin.
27.
Pathogenicity
• Source ofinfection
Exogenous : patient or carrier
Endogenous : from colonized site
• Mode of Transmission
Contact : direct/indirect through fomites
Inhalation : Air borne droplets
28.
CLINICAL FEATURES
• S– Soft tissue infections i.e. folliculitis, impetigo
• O – Osteomyelitis , musculoskeletal infections
• F – Food poisoning
• T – TSST, TEN
• P – Pneuminia
• A – Acute endocarditis
• I – Infective arthritis
• N – Necrotising fascitis
• S - Sepsis
29.
Acute endocarditis
• (ifperson <12month= S.epidermidis & >12 month = S.viridians)
• In I.V drug abusers then right side of heart –S. aureus & left side of
heart – Enterococcus
30.
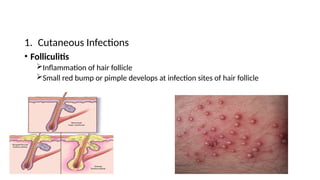
1. Cutaneous Infections
•Folliculitis
Inflammation of hair follicle
Small red bump or pimple develops at infection sites of hair follicle
31.
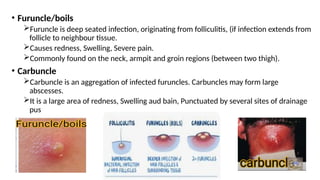
• Furuncle/boils
Furuncle isdeep seated infection, originating from folliculitis, (if infection extends from
follicle to neighbour tissue.
Causes redness, Swelling, Severe pain.
Commonly found on the neck, armpit and groin regions (between two thigh).
• Carbuncle
Carbuncle is an aggregation of infected furuncles. Carbuncles may form large
abscesses.
It is a large area of redness, Swelling aud bain, Punctuated by several sites of drainage
pus
32.
• Impetigo
A verySuperficial Skin infection Common in Children, usually produces
blisters or Sores on the face, neck, hand and diapers area.
It is characterized by watery bristles, Which become pustules and then honey
Coloured Crust.
33.
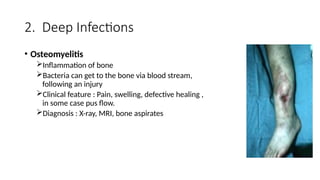
2. Deep Infections
•Osteomyelitis
Inflammation of bone
Bacteria can get to the bone via blood stream,
following an injury
Clinical feature : Pain, swelling, defective healing ,
in some case pus flow.
Diagnosis : X-ray, MRI, bone aspirates
34.
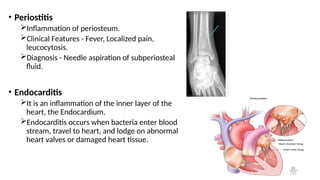
• Periostitis
Inflammation ofperiosteum.
Clinical Features - Fever, Localized pain,
leucocytosis.
Diagnosis - Needle aspiration of subperiosteal
fluid.
• Endocarditis
It is an inflammation of the inner layer of the
heart, the Endocardium.
Endocarditis occurs when bacteria enter blood
stream, travel to heart, and lodge on abnormal
heart valves or damaged heart tissue.
35.
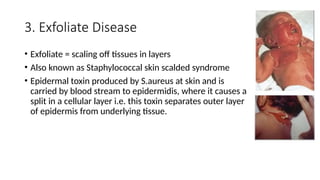
3. Exfoliate Disease
•Exfoliate = scaling off tissues in layers
• Also known as Staphylococcal skin scalded syndrome
• Epidermal toxin produced by S.aureus at skin and is
carried by blood stream to epidermidis, where it causes a
split in a cellular layer i.e. this toxin separates outer layer
of epidermis from underlying tissue.
36.
Types of SSSS:
Severeform Milder form
In new born - Ritter’s disease - Pemphigus neonatorum
In older patients - Toxic epidermal - Bullous ,necrolysis,
impetigo
37.
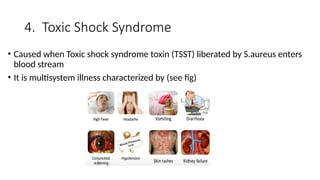
4. Toxic ShockSyndrome
• Caused when Toxic shock syndrome toxin (TSST) liberated by S.aureus enters
blood stream
• It is multisystem illness characterized by (see fig)
38.
2) Staphylococcal Toxicshock syndrome (STSS):
• STSS is associated with infection of mucosal or sequestered sites by
TSST( formerly known as enterotoxin type F) producing S.aureus.
• It is fatal multisystem disease presenting with fever, hypotension,
myalgia, vomiting, diarrhea, mucosal hyperemia and erythematous
rash which desquamates subsequently.
39.
2 types ofSTSS known:
i) Menstrual associated STSS: Here colonization of S.aureus occurs in
the vagina of menstruating woman who uses highly absorbent vaginal
tampons.
ii) Non menstrual associated STSS: Here colonization of S.aureus occurs
in other sites like surgical wound.
40.
5. Staphylococcal FoodPoisoning
• Caused when consuming food in which S.aureus has multiplied and
formed endotoxin.
• Symptoms : Nausea, vomiting, Severe abdominal cramp, Diarrhoea,
Sweating, Headache etc.
• Mode of Transmission : Person with lesions, Air borne droplets,
Asymptomatic carrier, Cross-Infection
41.
Epidemiology
• Human patientsand carriers are the commonest source of infection.
• In hospital, more than 50% of nursing staff are carriers of
Staphylococcus aureus.
• Staphyloccal disease may be exogenous & endogenous.
• Staphylococci are the commonest cause of hospital cross infection.
42.
Prevention
• Isolation &treatment of MRSA patients
• Detection of carriers among hospital staff, their isolation &
treatment.
• Avoid indiscriminate usage of antibiotics.
• Stop misuse of antibiotics.
43.
Treatment
• Drug resistanceis common.
• Benzyl penicillin most effective antibiotic, if the strain is sensitive.
• Cloxacillin or methicillin used against B-Lactamase.
• Vancomycin is used in treatment of infection with MRSA. (Harboring
vanA & me CA).
• Tolerance to penicillin.
44.
Laboratory Diagnosis
• HematologicalInvestigation
TLC ( Normal = 4,000 – 10,000 cells/mm3
, In infection >10,000 cells/mm3
)
DLC (Normal = 80%, Infection = >80%)
• Bacteriological Investigation
Specimens
o Pus : from wound or abscess or burns
o Nasal swab : from suspected carrier
o Food : To diagnose staphylococcal intoxication
o Blood : To diagnose endocarditis and bacteremia
o Sputum : To diagnose lower respiratory tract infection
o Urine : UTI
o CSF : meningitis
o Feces : Food poisoning
o Food or vomit : Food poisoning
45.
Collection & Transport
DirectMicroscopy
Culture
Colony morphology & Gram staining
Biochemical rxns
oCatalase – positive , Cagulase – positive
oMannitol fermentation – Acid production without gas
oGelatin liquefaction – positive
oTellunite reduction – positive
oProduction of enzyme phosphatase
oOxidase – Negative
oDNAse – Positive
Bacteriophage typing
46.
References
• Ananthnarayan andPanikers Textbook of Microbiology
• Apurba Sankar Sastry and Sandhya Bhat - Essentials of Medical
Microbiology-Jaypee Brothers Medical Publishers
• Textbook of Microbiology – Dr. C.P. Baveja