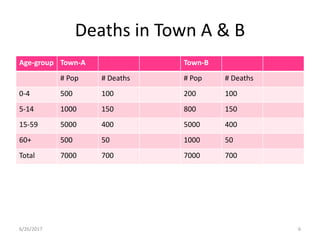
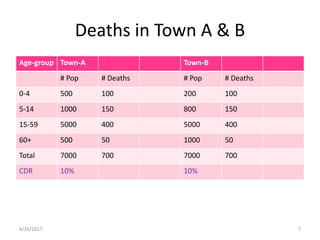
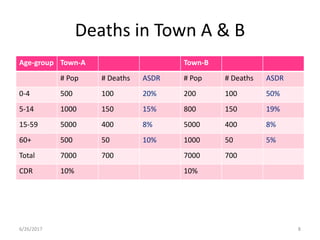
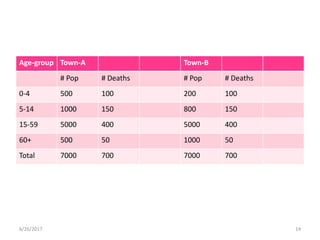
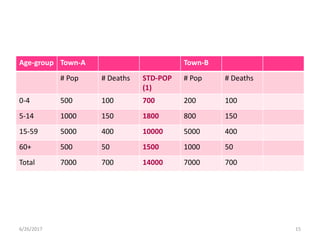
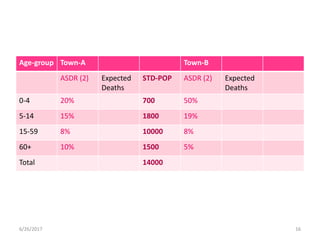
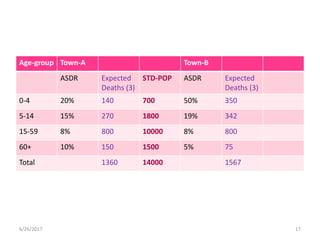
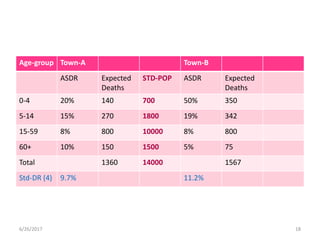
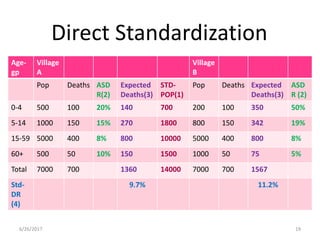
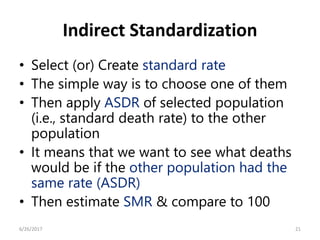
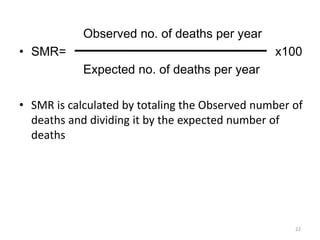
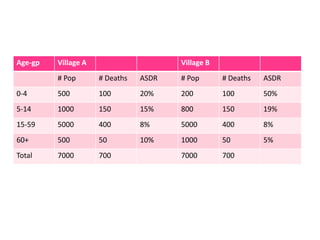
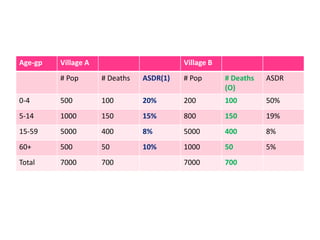
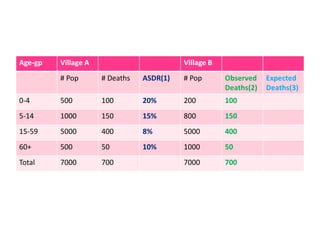
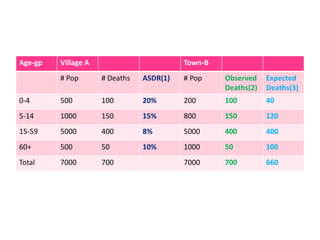
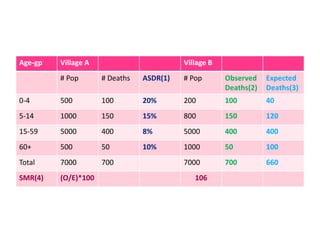
This document discusses methods for standardizing mortality rates to account for differences in population age distributions. Direct standardization uses a standard population to calculate expected mortality rates. Indirect standardization calculates a standardized mortality ratio (SMR) by comparing observed deaths to expected deaths based on a reference population's age-specific death rates. Direct standardization allows comparing absolute mortality rates while indirect standardization expresses differences as a ratio. Standardization is necessary when comparing populations that differ in their age structures.