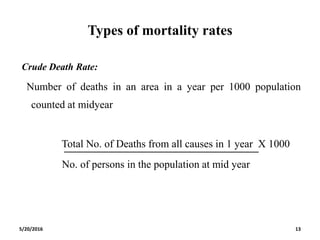
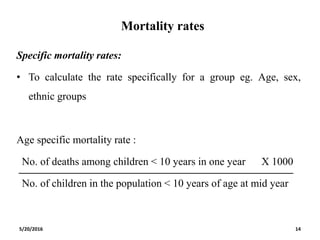
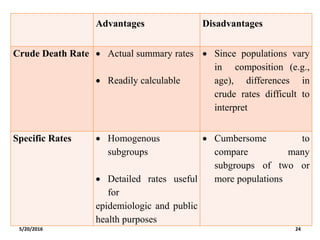
The document discusses mortality rates, their definitions, and types, including crude, specific, case fatality, and proportional mortality rates. It highlights the relevance of mortality rates in public health for indicating health problems and disease severity, and addresses standardization techniques for comparing mortality data across populations. Additionally, the document explores the advantages and limitations of different mortality data types and methodologies for calculating and interpreting these rates.
![References
• Age standardization of rates: A new WHO standard. World Health
Organisation [online] 2001 [cited on 2016 May 1];Available from:
URL: http://www.who.int/healthinfo/paper31.pdf
• The use of epidemiological tools in conflict affected populations:
open access educational resources for policymakers. World Health
Organisation [online] 2002 [cited on 2016 Apr 24]; Available from:
URL:http://www.who.int/hac/techguidance/tools/disrupted_sectors/a
dhsm_mod14_en.pdf
5/20/2016 70](https://image.slidesharecdn.com/mortalitystandardization-160520100034/85/Mortality-rates-standardization-69-320.jpg)
![References
• Standardization of rates and ratios. Concepts and basic methods for
deriving measures that are comparable across populations that differ
in age and other demographic variables [Online] [ cited on 2016 Apr
20];Available from: URL:
http://www.epidemiolog.net/evolving/Standardization.pdf
• West MD, Kanchanaraksa S. The Direct and Indirect Methods of
Adjustment. John Hopkins School of Public Health [online] [cited
on 2016 Apr 23]; Available from: URL:
http://ocw.jhsph.edu/courses/fundepi/PDFs/Lecture7.pdf
5/20/2016 71](https://image.slidesharecdn.com/mortalitystandardization-160520100034/85/Mortality-rates-standardization-70-320.jpg)
![References
• Standardization of rates. Boston University School of Public Health
[online] 2006 [Cited 2016 Apr 21]; Available from: URL:
http://sphweb.bumc.bu.edu/otlt/MPH-
Modules/PH/Woburn/Woburn8.html
• Curtin LR, Klein RJ. Direct Standardization (Age-Adjusted Death
Rates). Healthy People 2000. CDC [Online] 1995 [Cited on 2016
Apr 24]; Available from: URL:
www.cdc.gov/nchs/data/statnt/statnt06rv.pdf
5/20/2016 72](https://image.slidesharecdn.com/mortalitystandardization-160520100034/85/Mortality-rates-standardization-71-320.jpg)