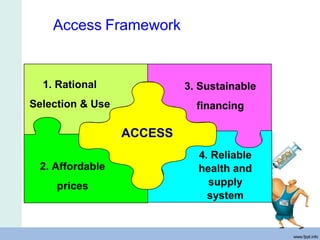
The Myanmar Essential Medicines Project aims to ensure regular access to safe, effective, and affordable essential medicines. It was started in 1988 and has now covered all townships. Major activities include building human resource capacity, reviewing treatment guidelines, and integrating essential medicines concepts into university curricula. Future plans include further education and promoting rational medicine use. Essential medicines are those that meet a population's priority healthcare needs and should be continuously available at a cost people can afford. The concepts of essential medicines focus on access, quality, and rational medicine use.