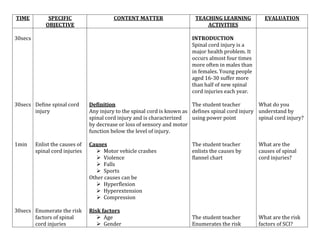
- Spinal cord injuries occur most often in males aged 16-30 and result from motor vehicle accidents, violence, falls, or sports.
- Medical management includes immobilizing the spine, administering steroids to reduce swelling, and surgery to decompress the spinal cord if needed.
- Nursing management focuses on respiratory care if needed, skin integrity, bowel and bladder care, pain management, and preventing complications like infection, blood clots, and autonomic dysreflexia.





![Spinal cord injury [recovered]](https://cdn.slidesharecdn.com/ss_thumbnails/spinalcordinjuryrecovered-201022180848-thumbnail.jpg?width=640&height=640&fit=bounds)






























![9 Spinal Cord Injury Sci [2]](https://cdn.slidesharecdn.com/ss_thumbnails/9spinalcordinjurysci2-100330221058-phpapp01-thumbnail.jpg?width=640&height=640&fit=bounds)























































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)




![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)






