Downloaded 3,111 times
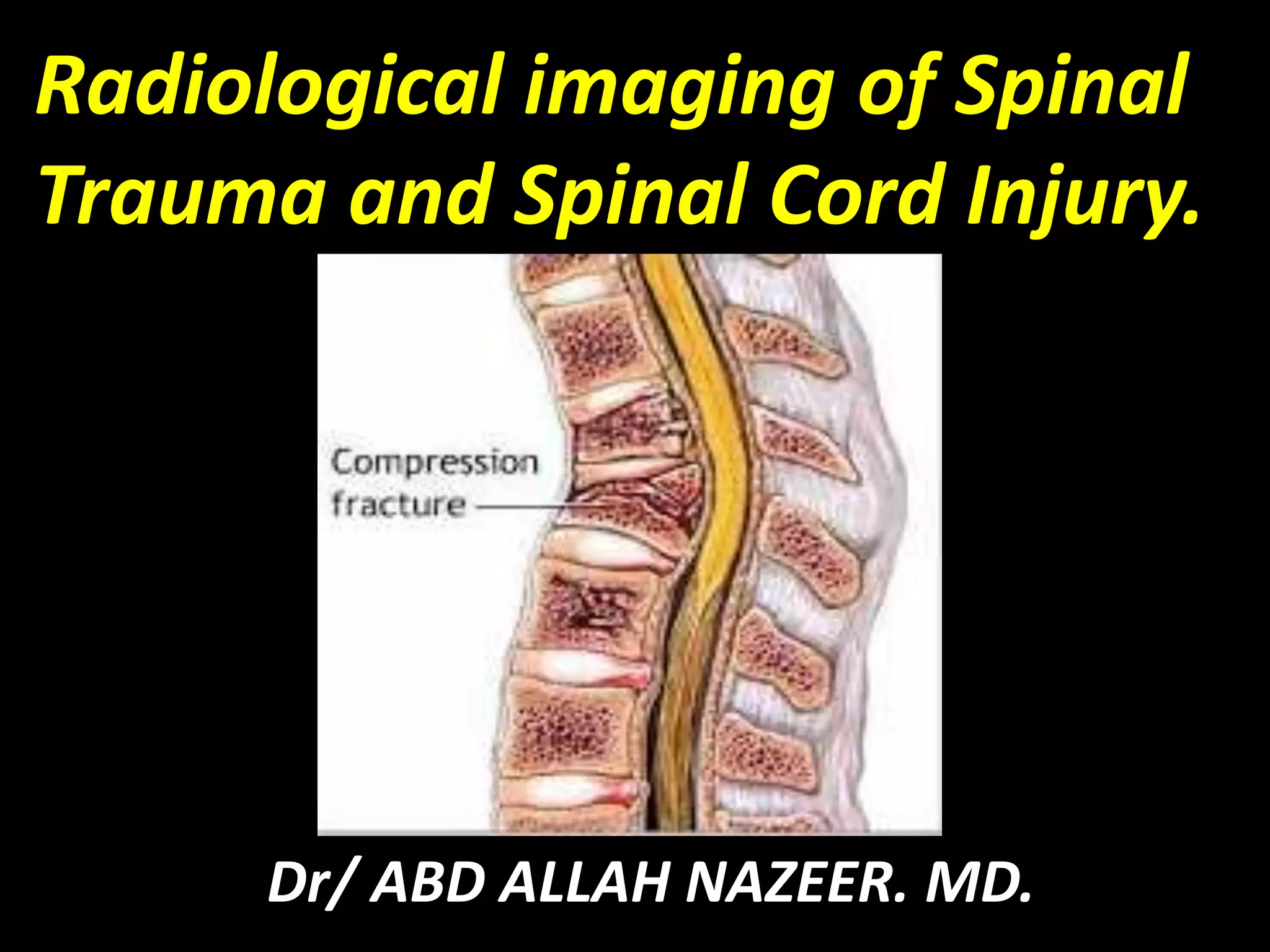
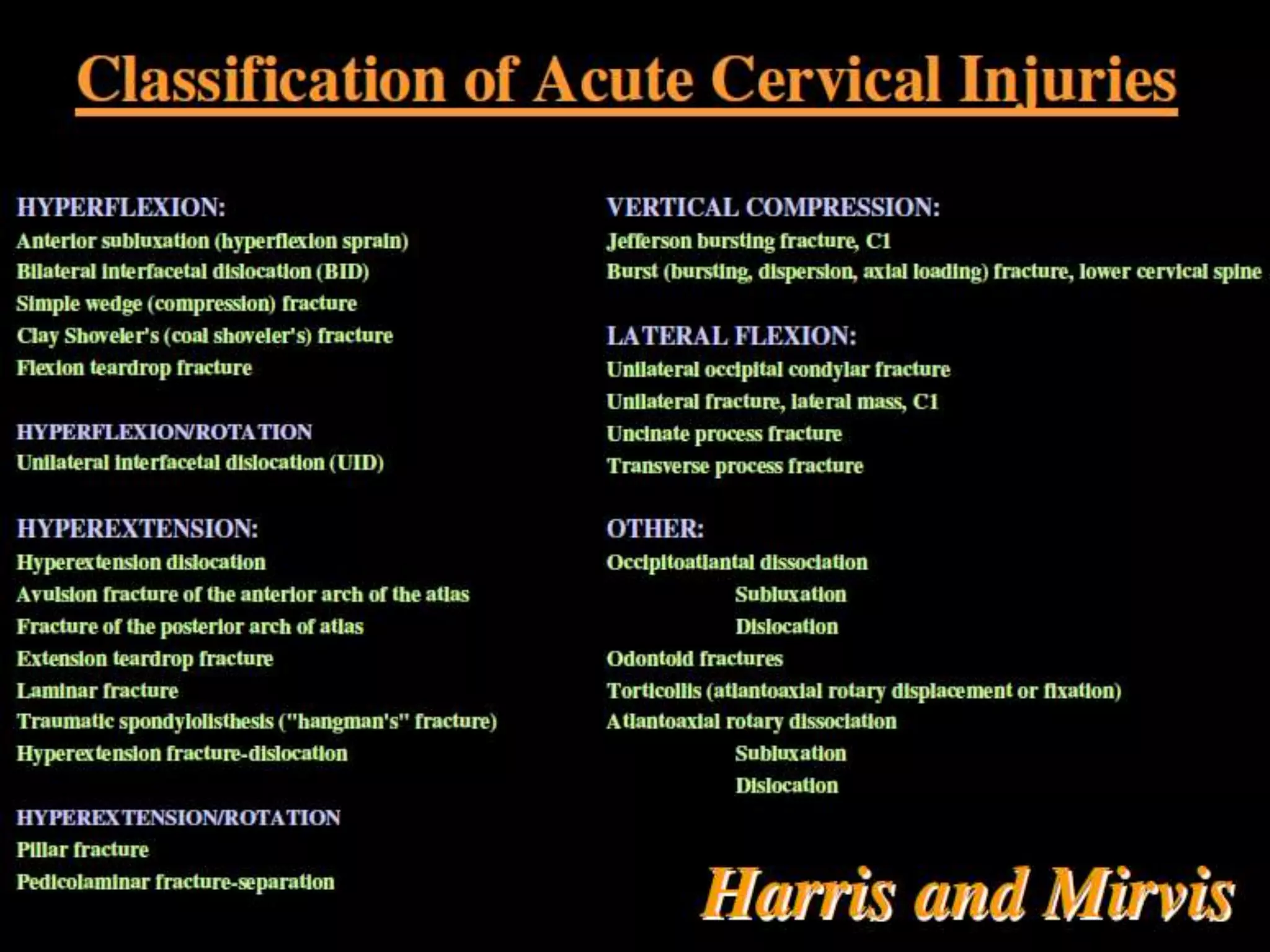
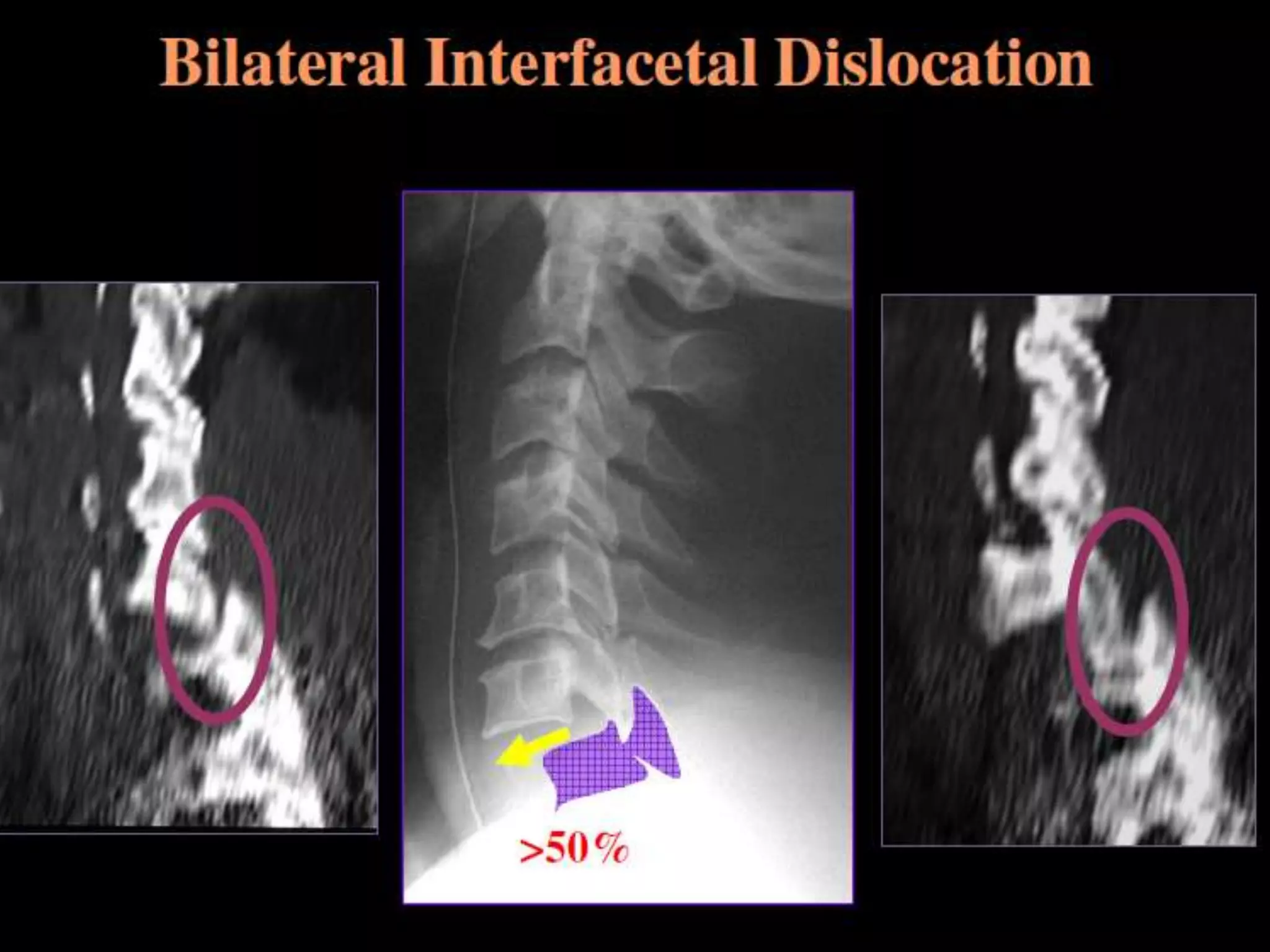
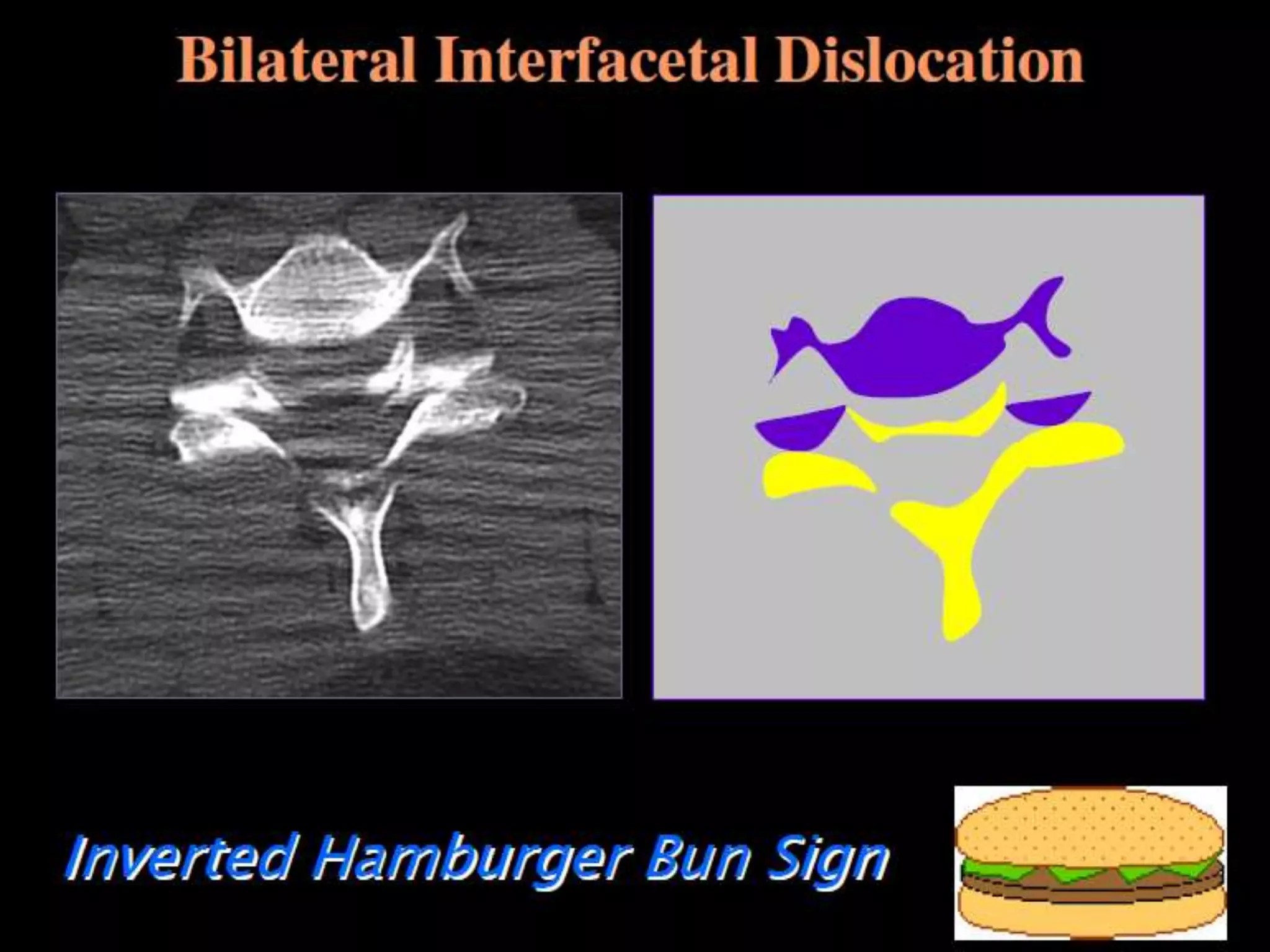
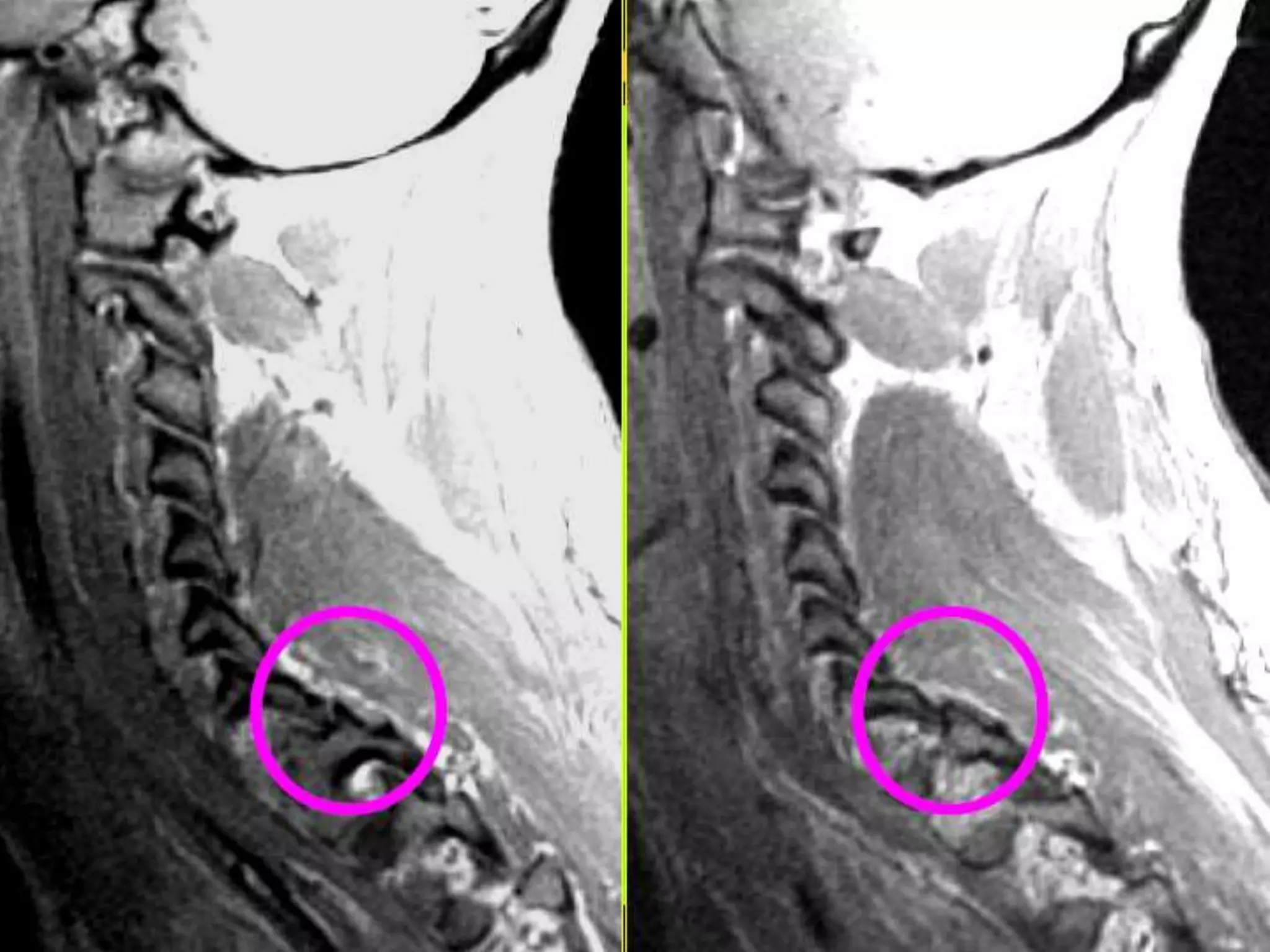
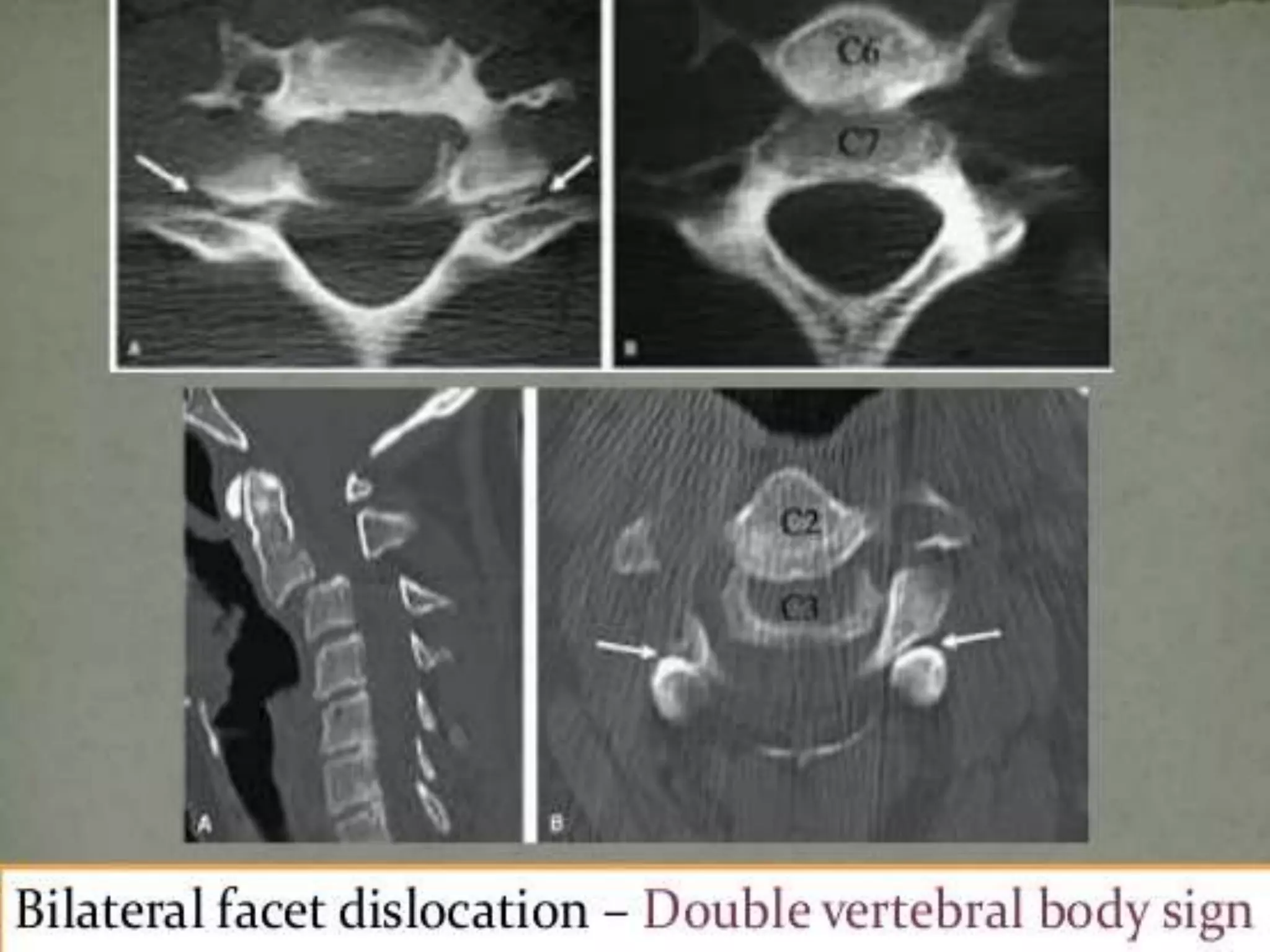




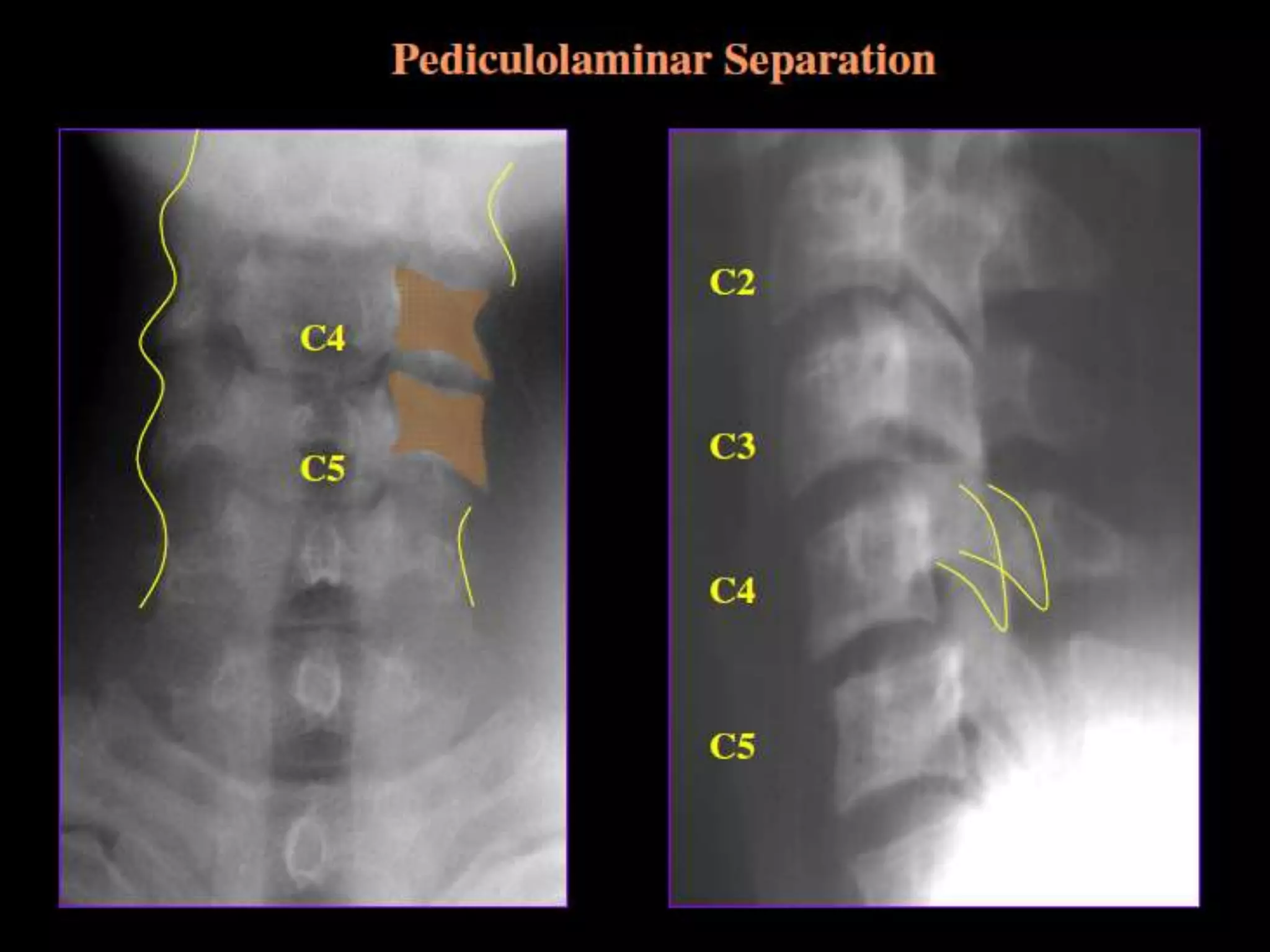
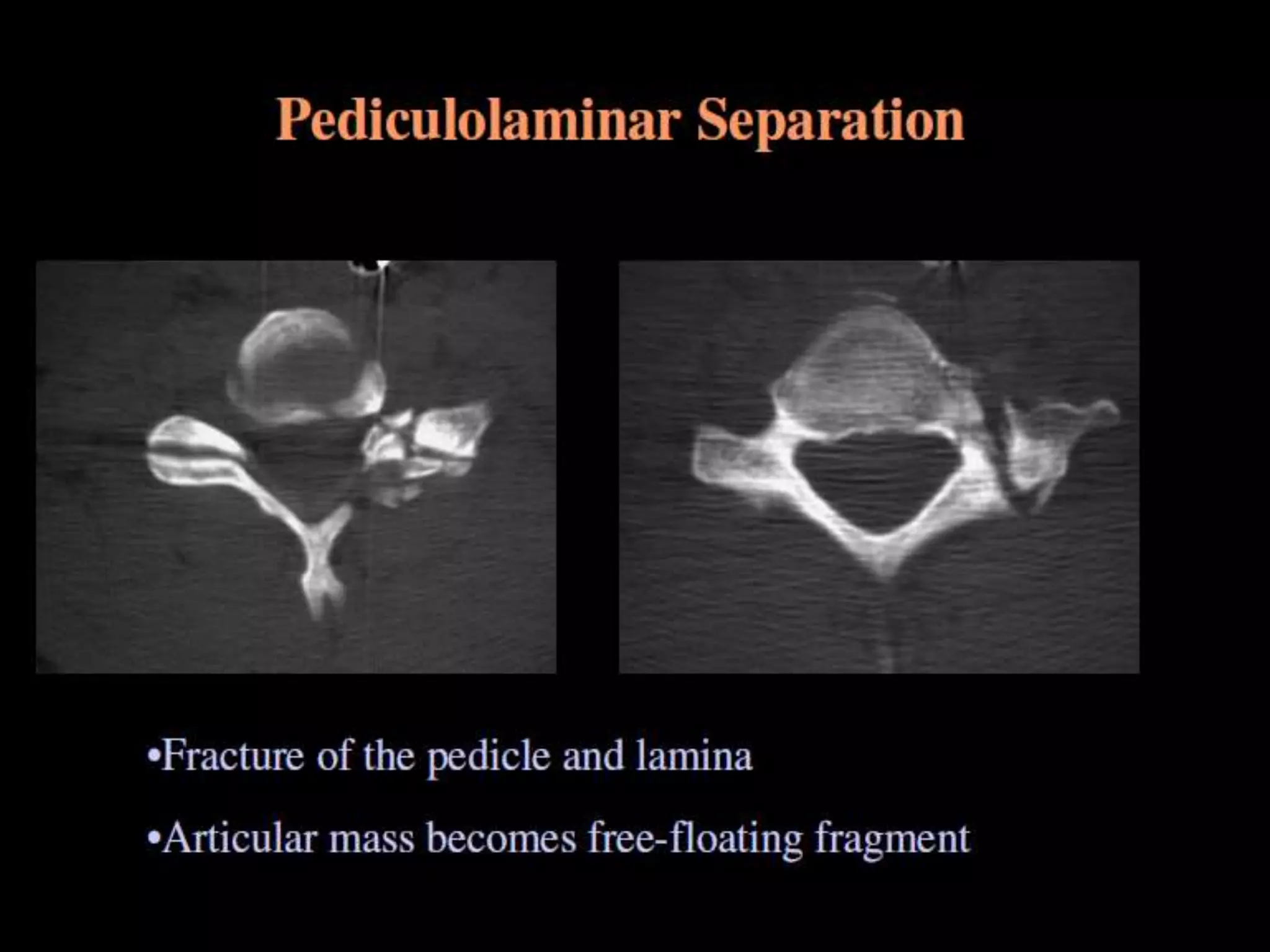
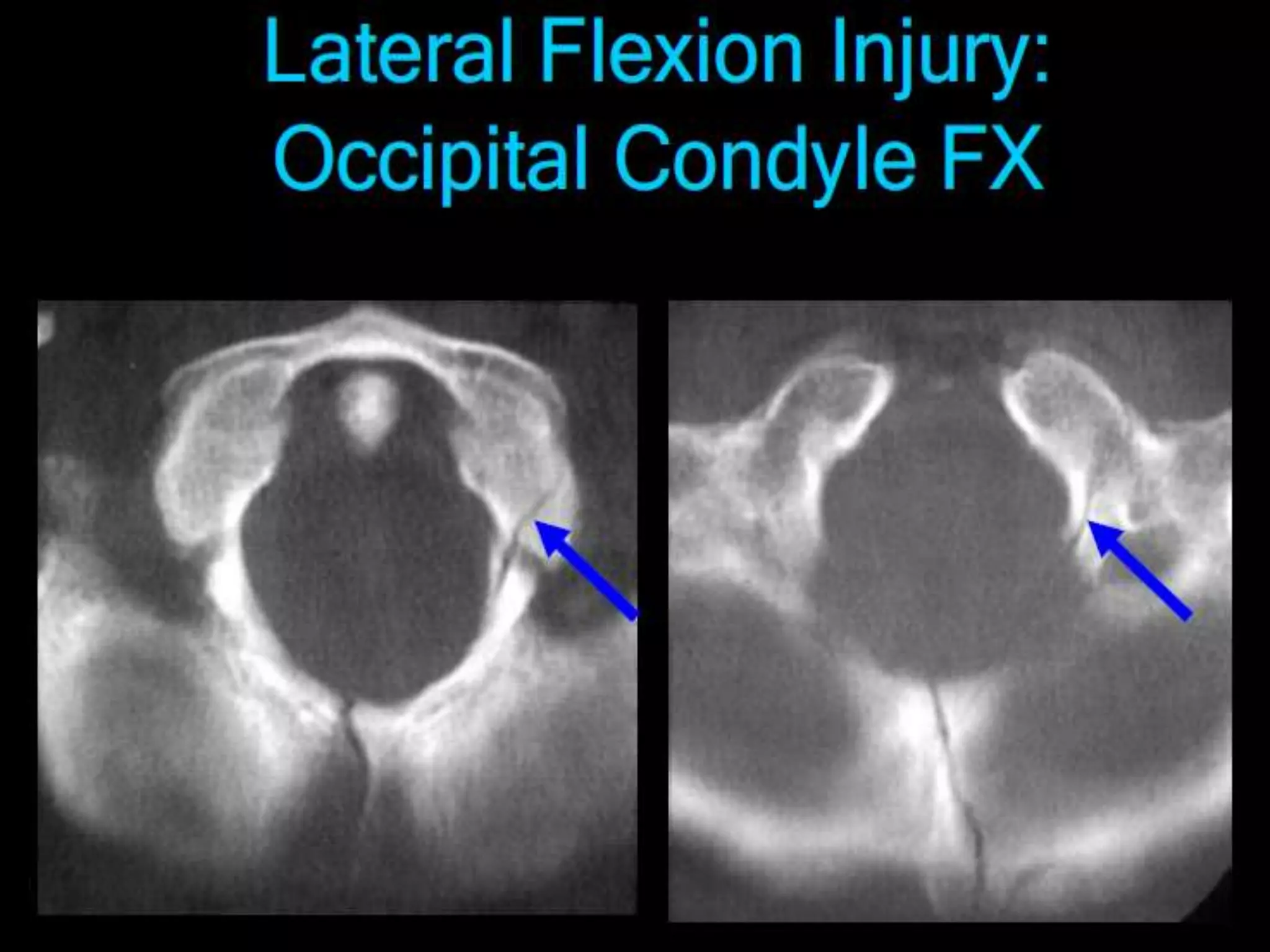
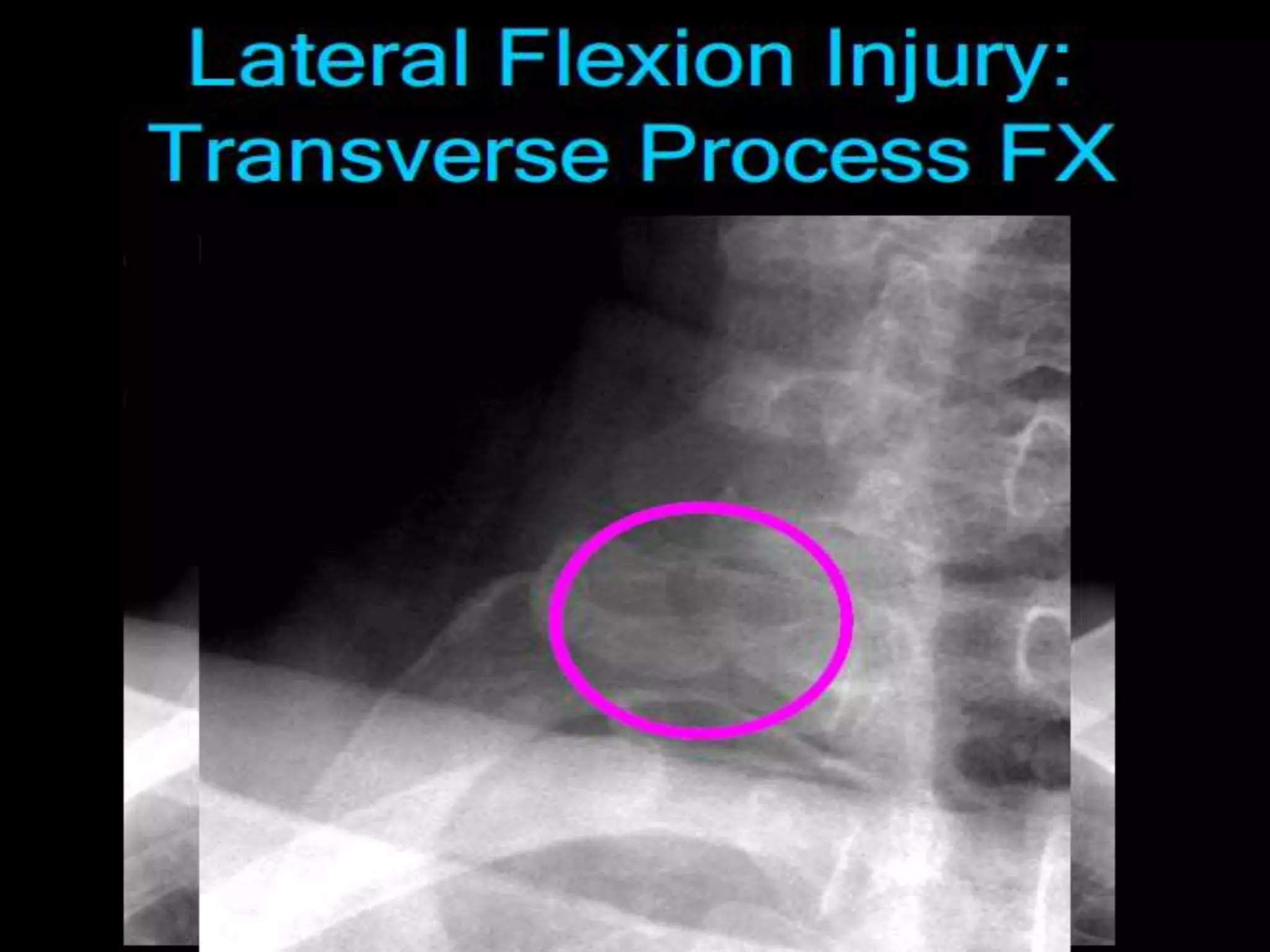
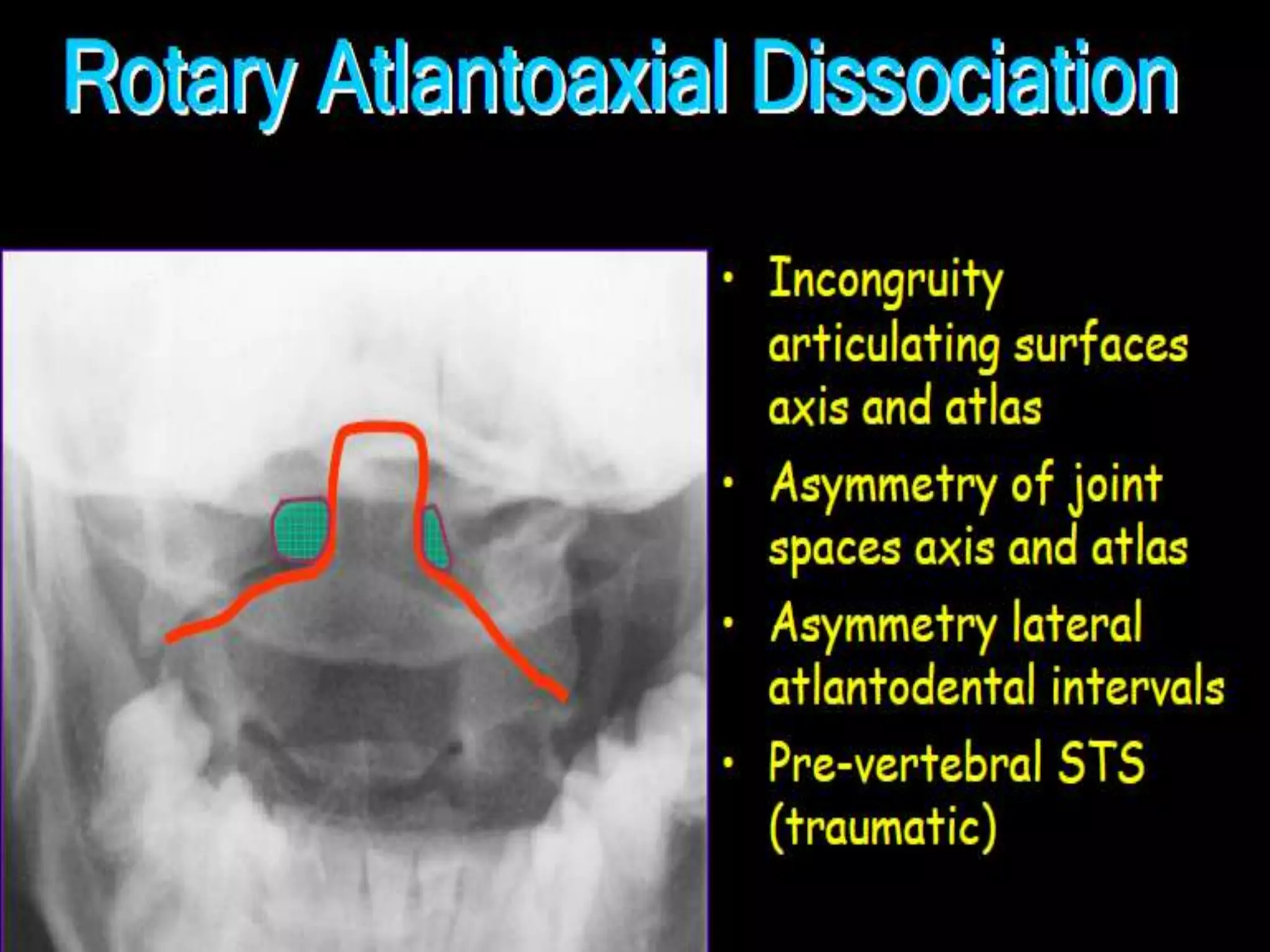
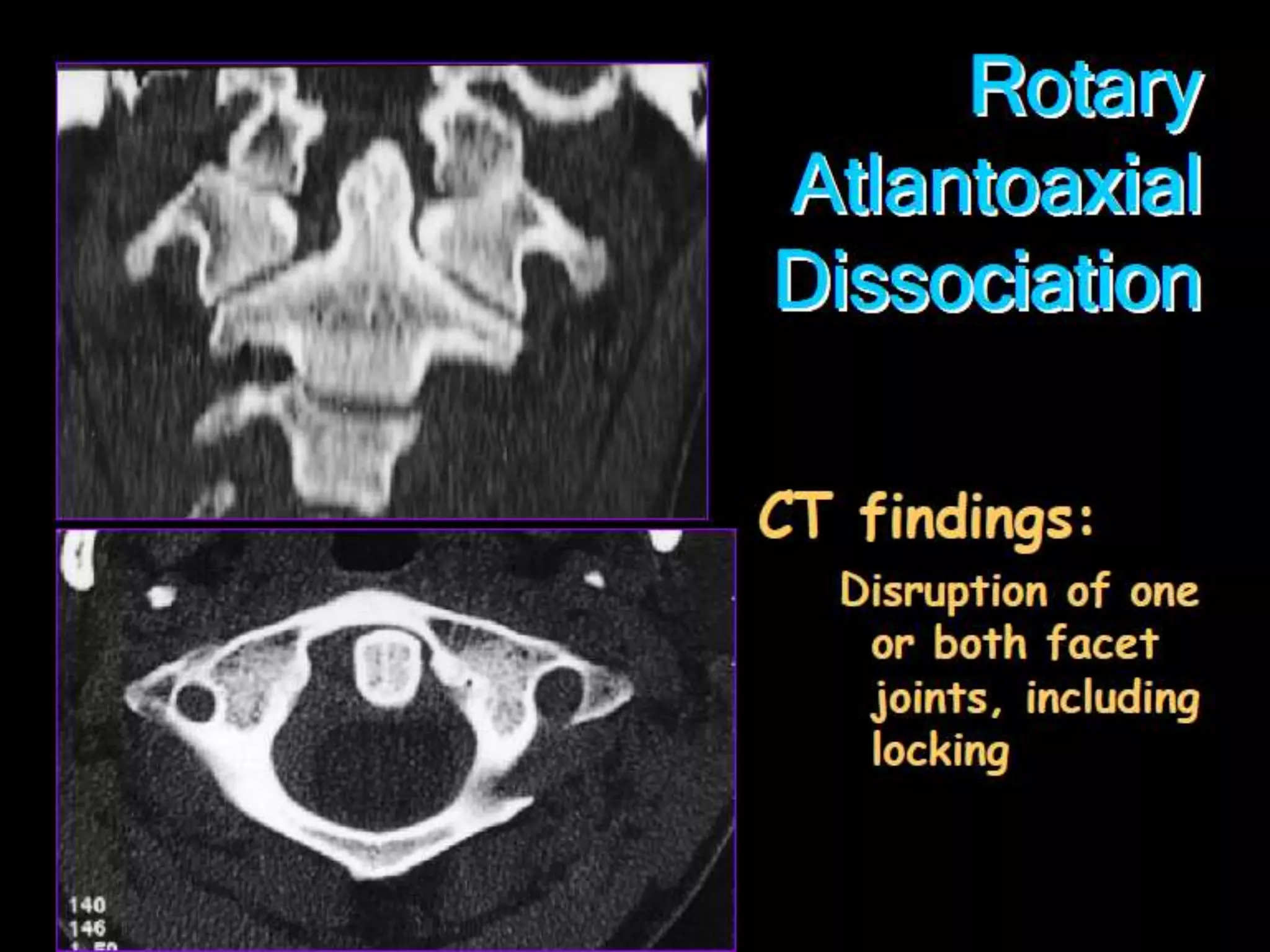
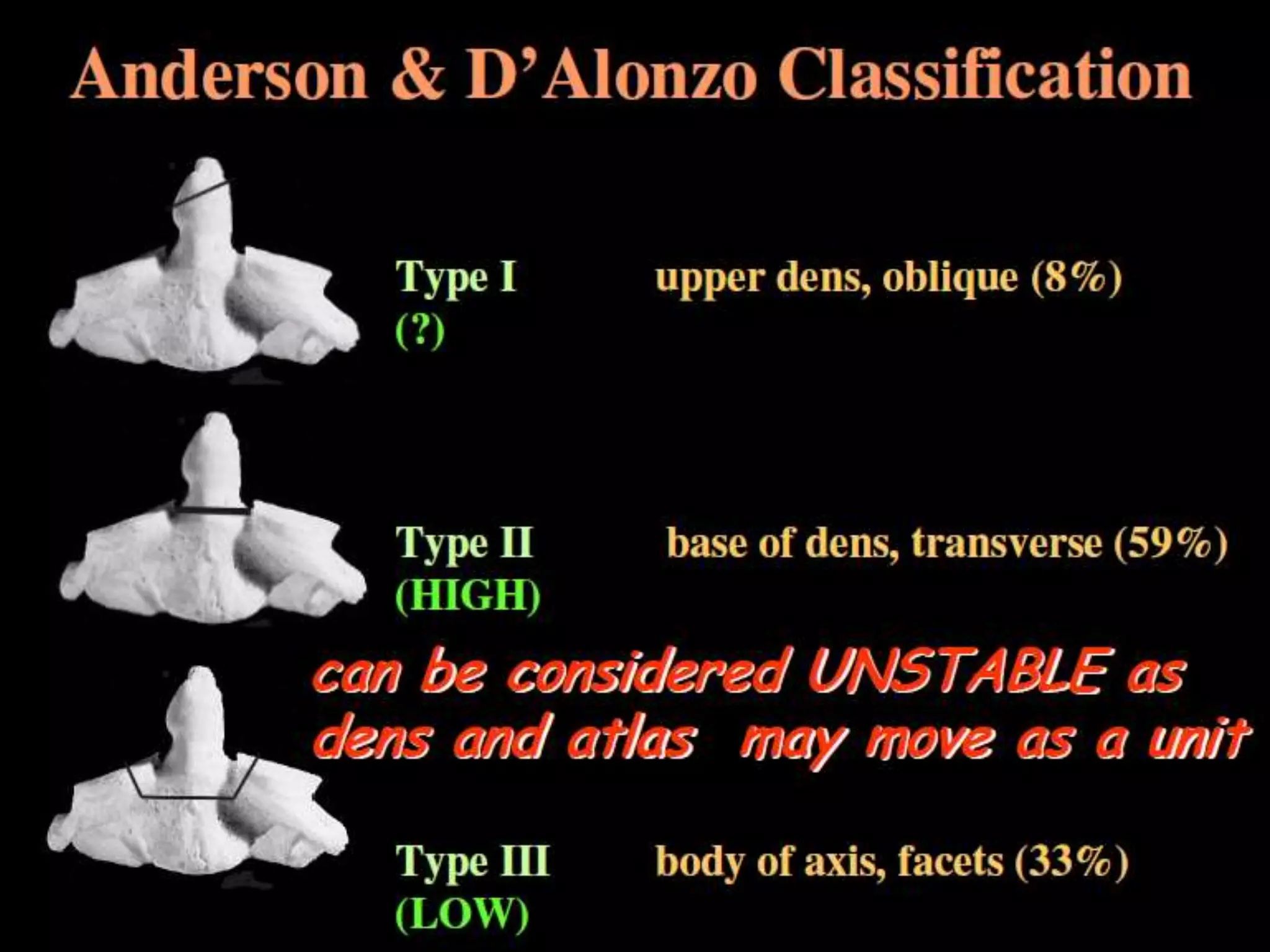
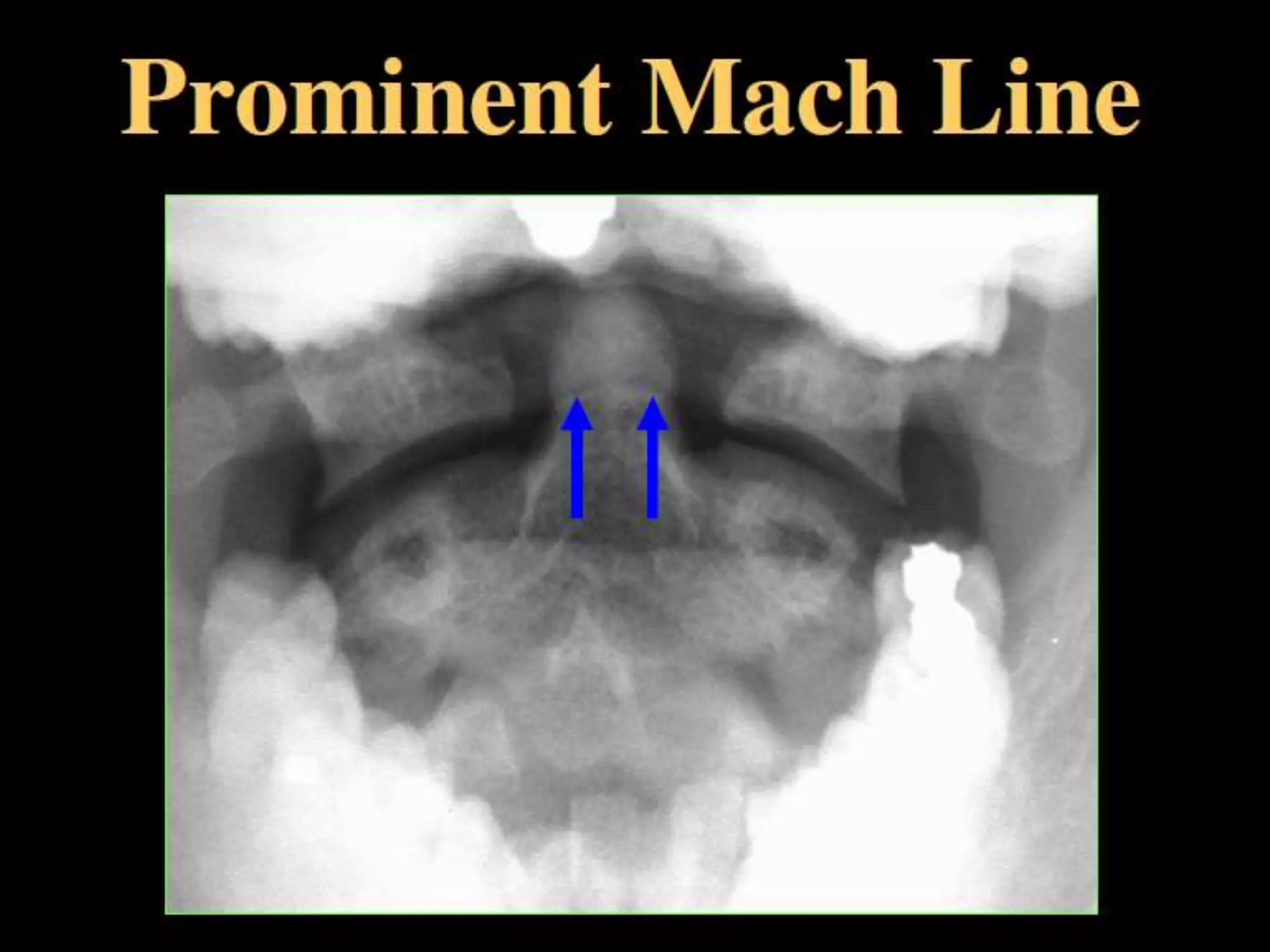
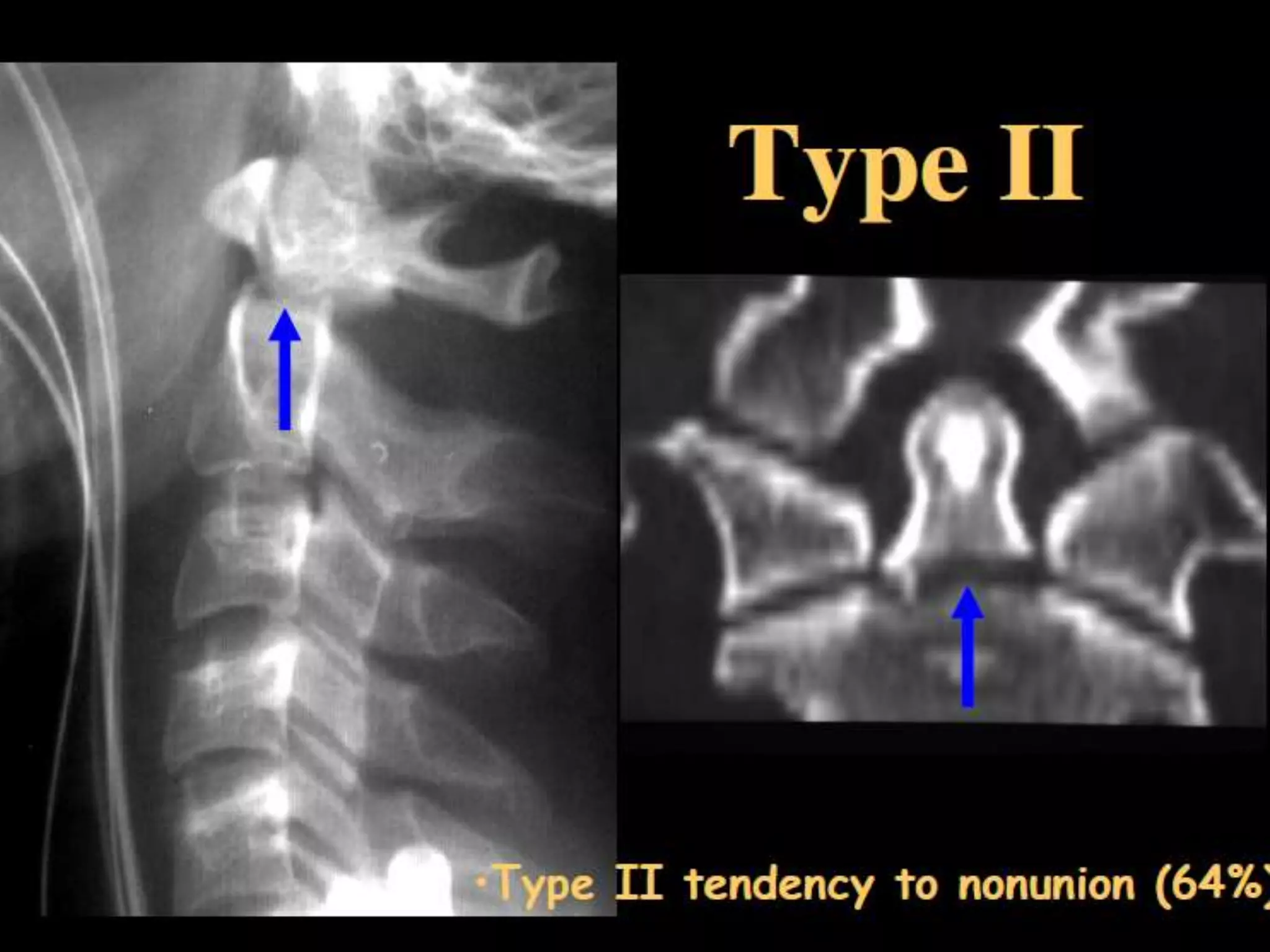
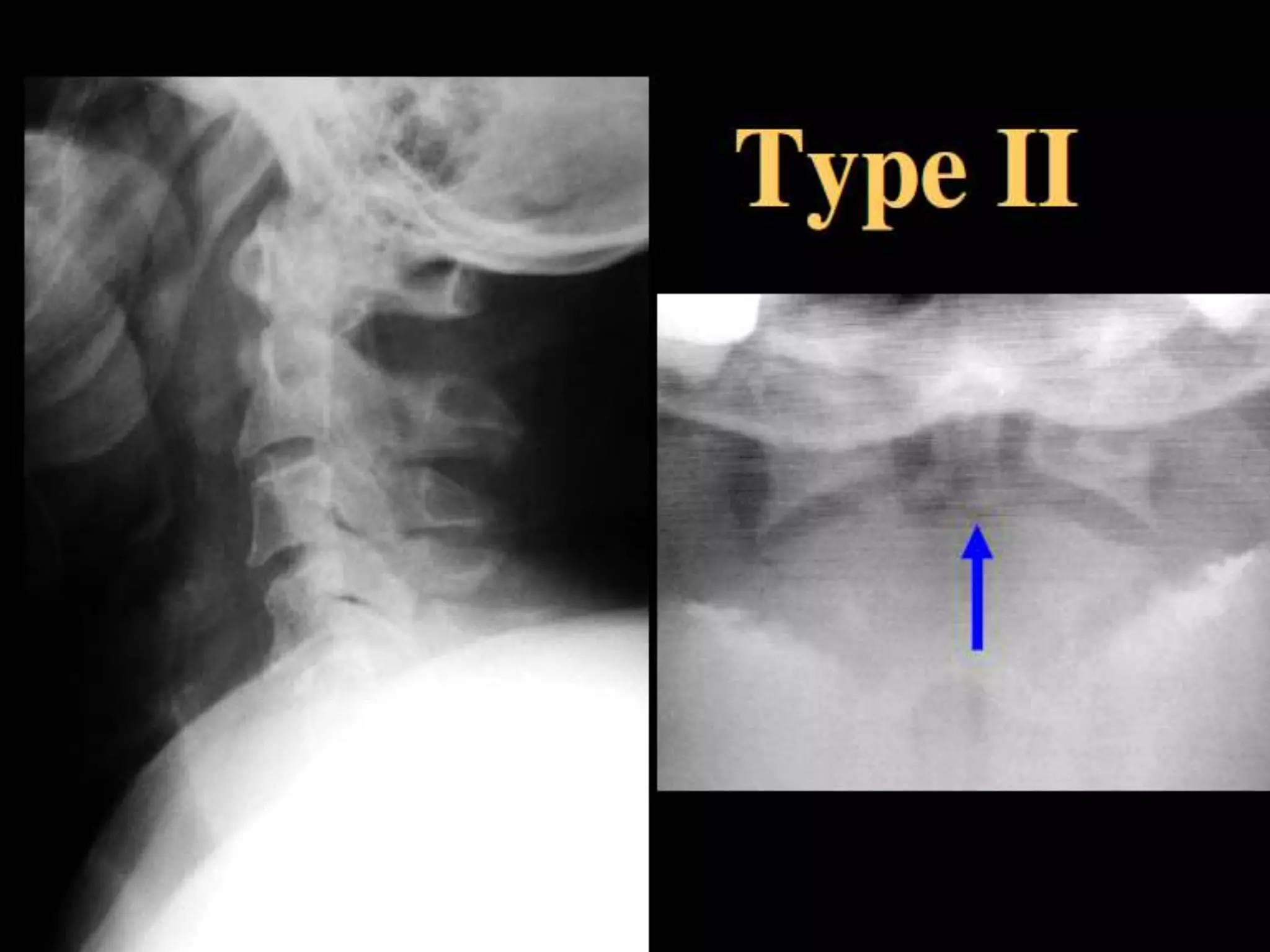
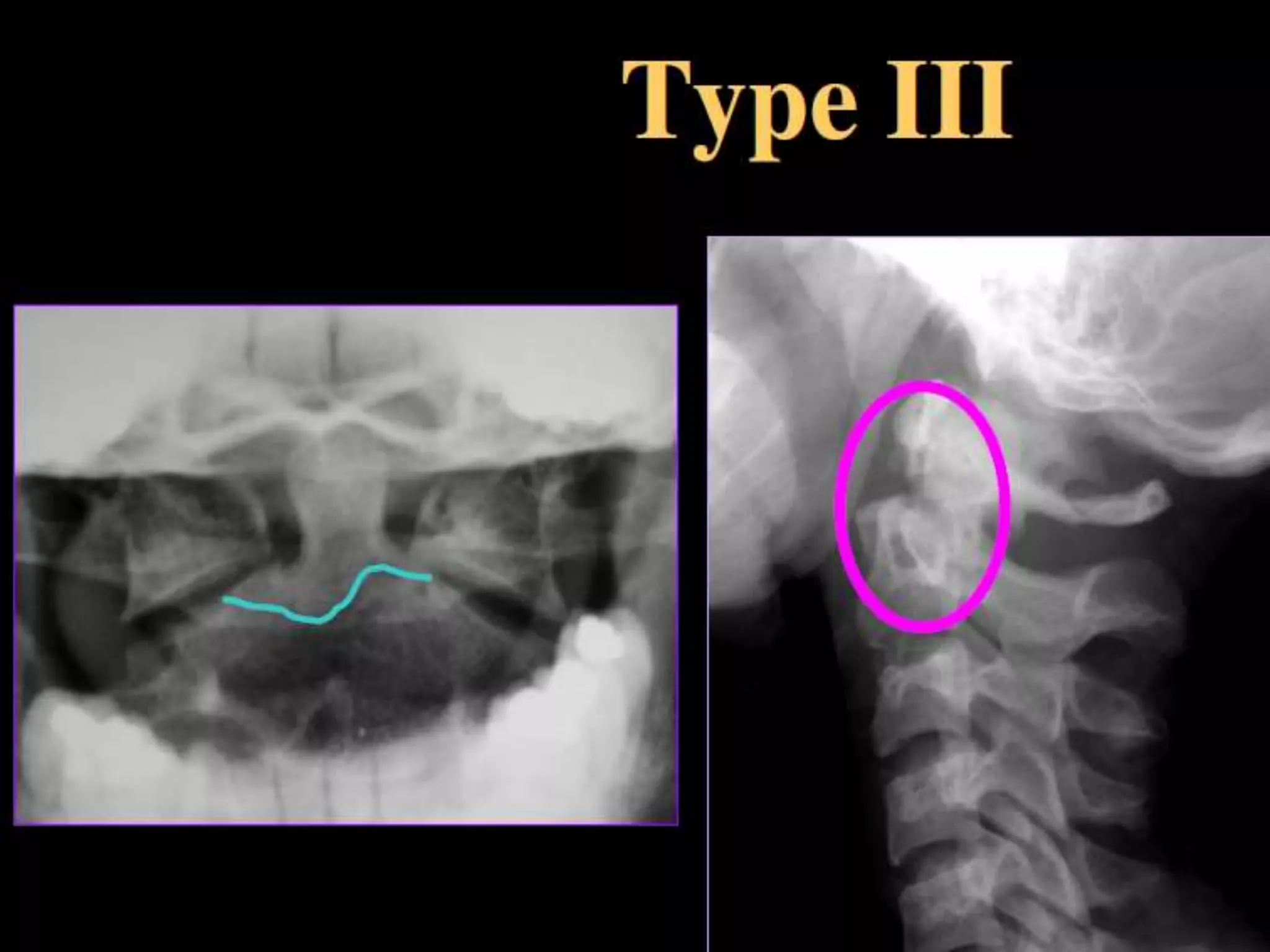
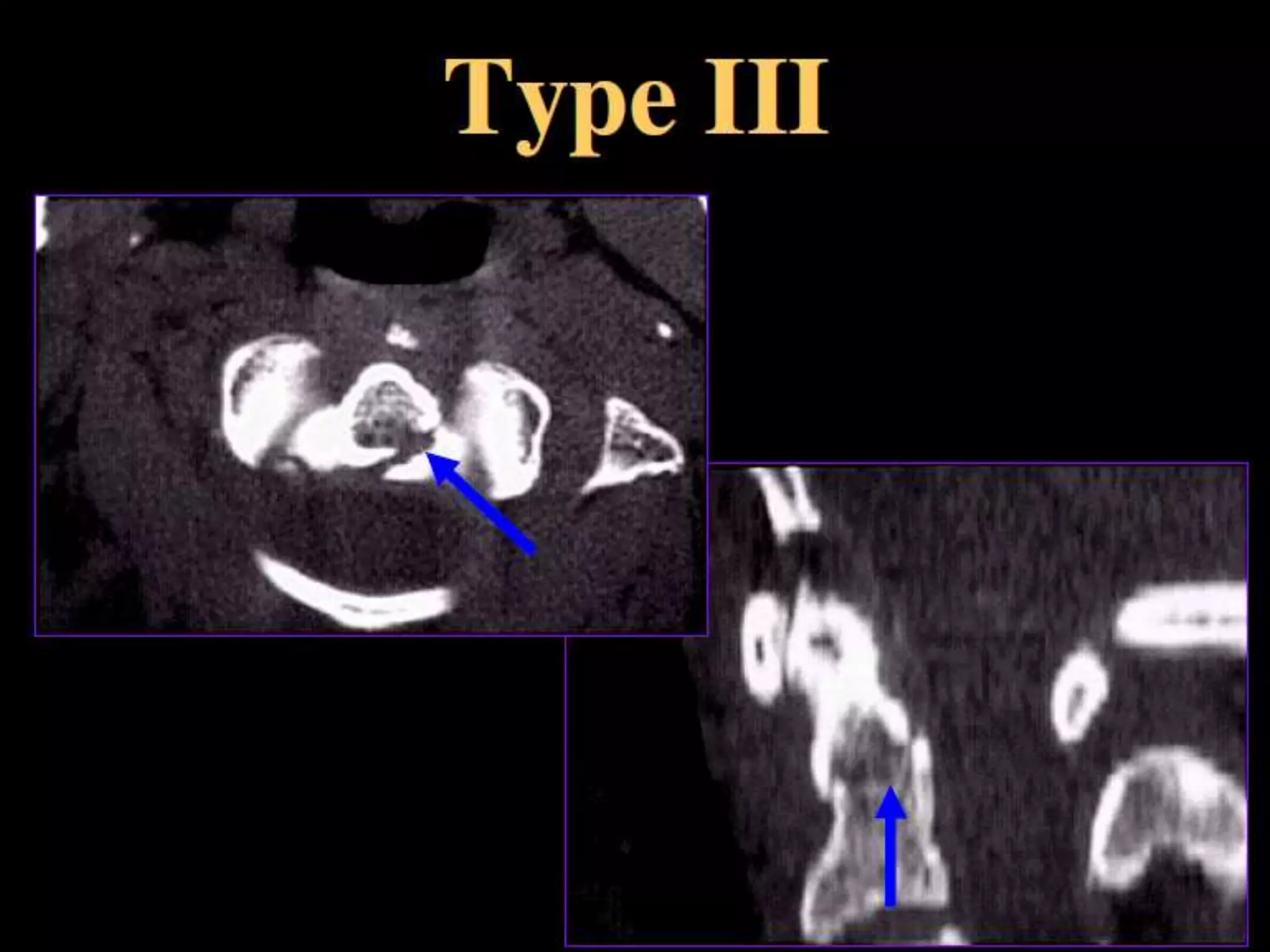
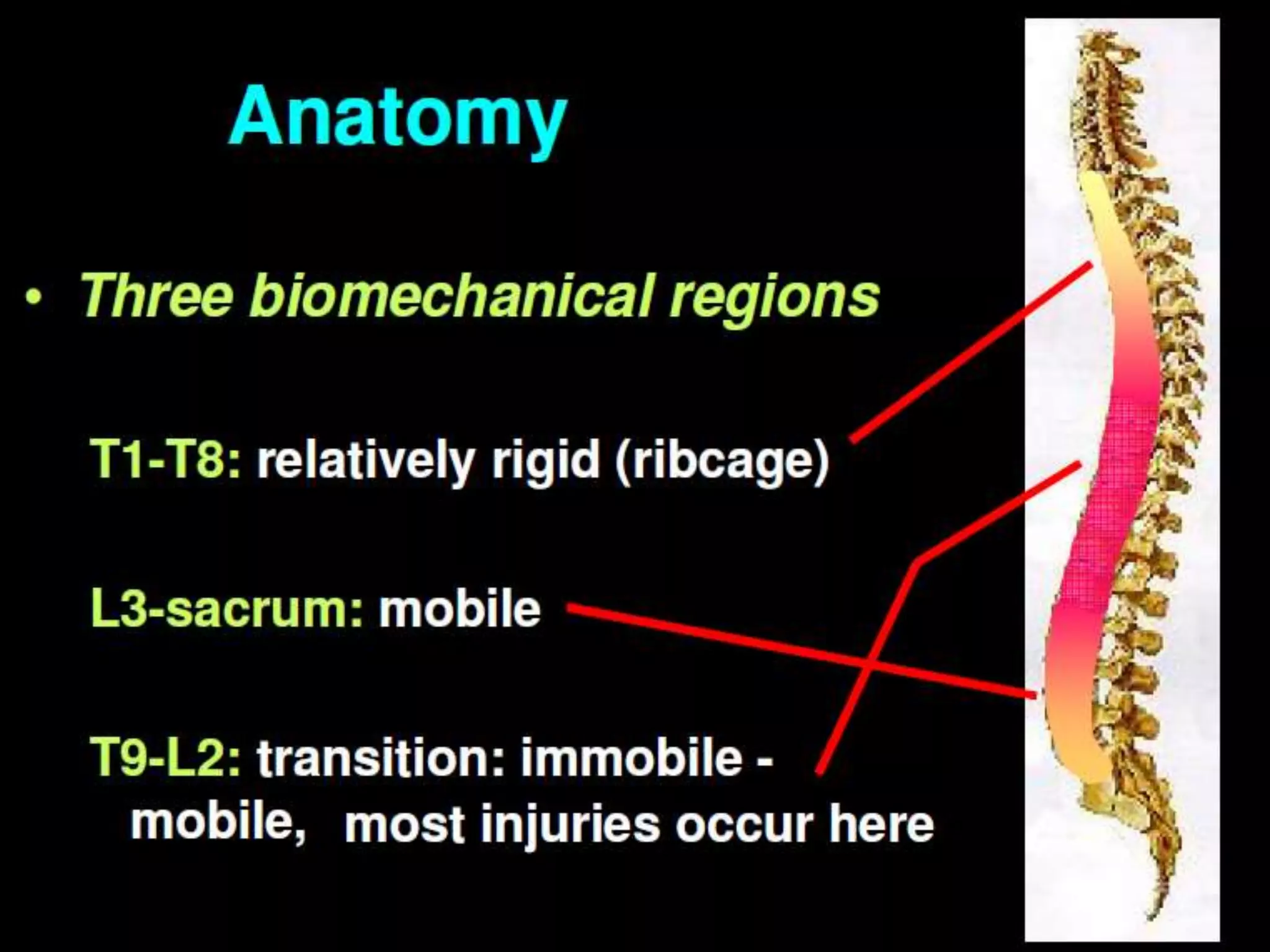
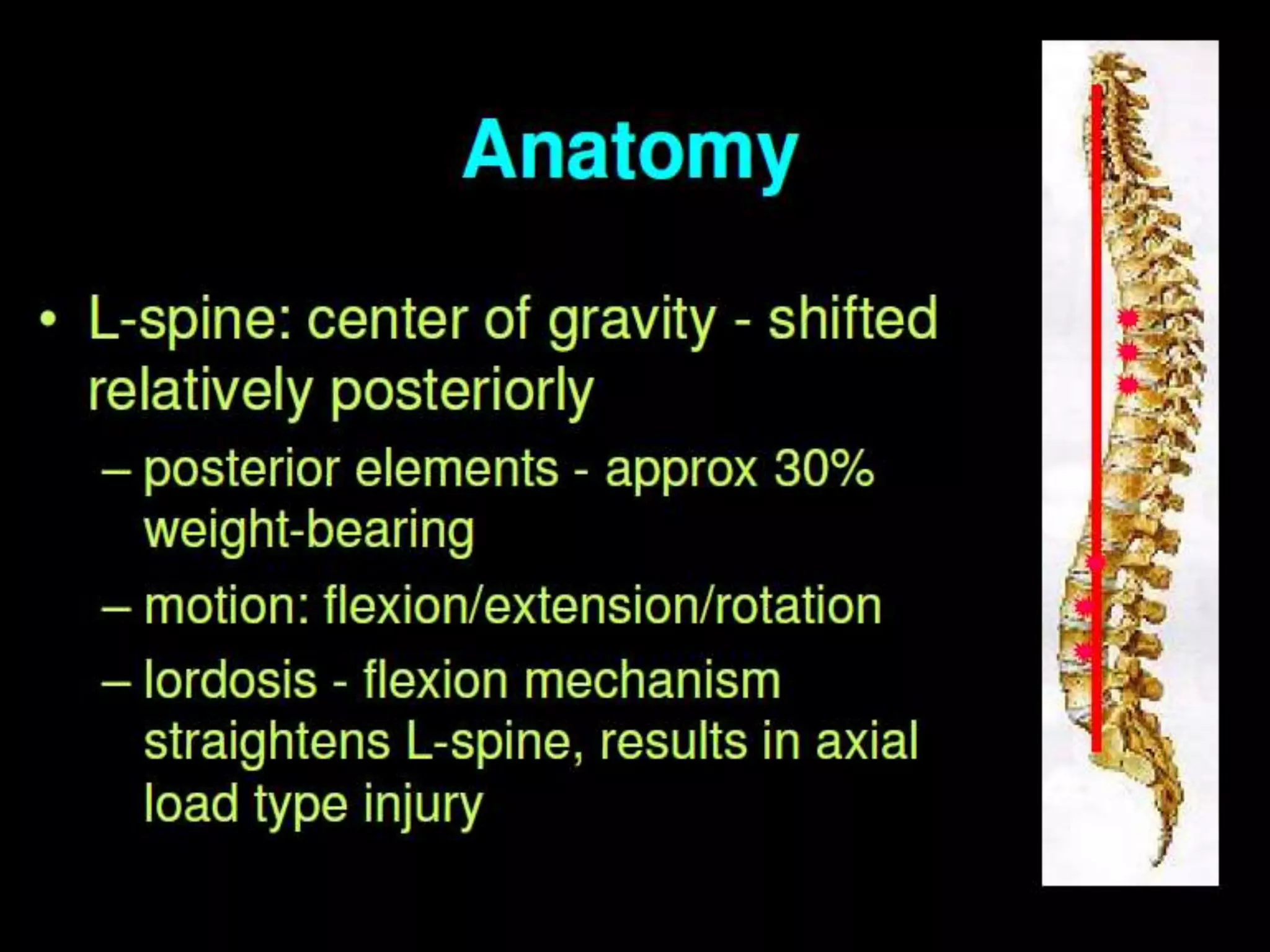
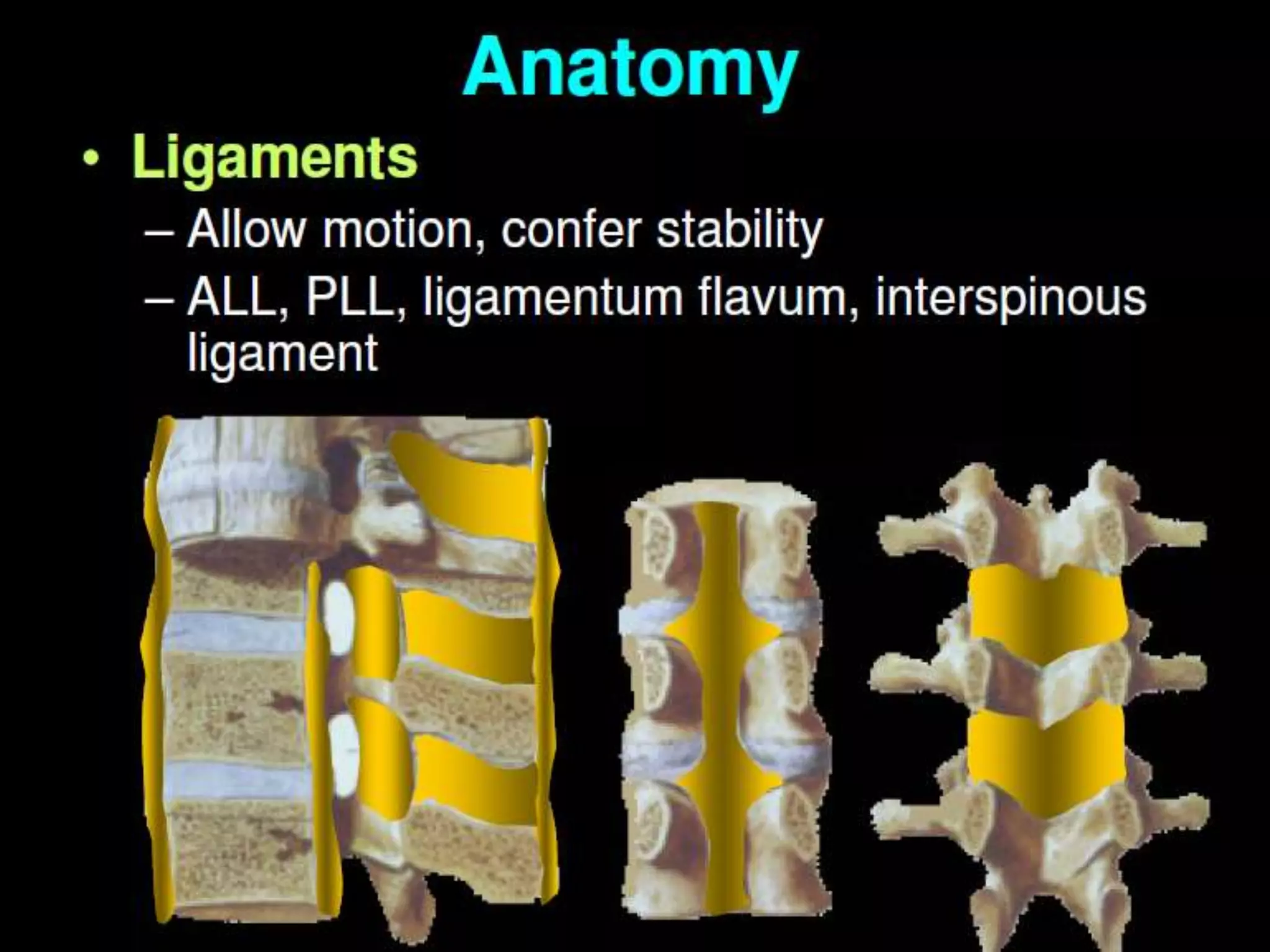
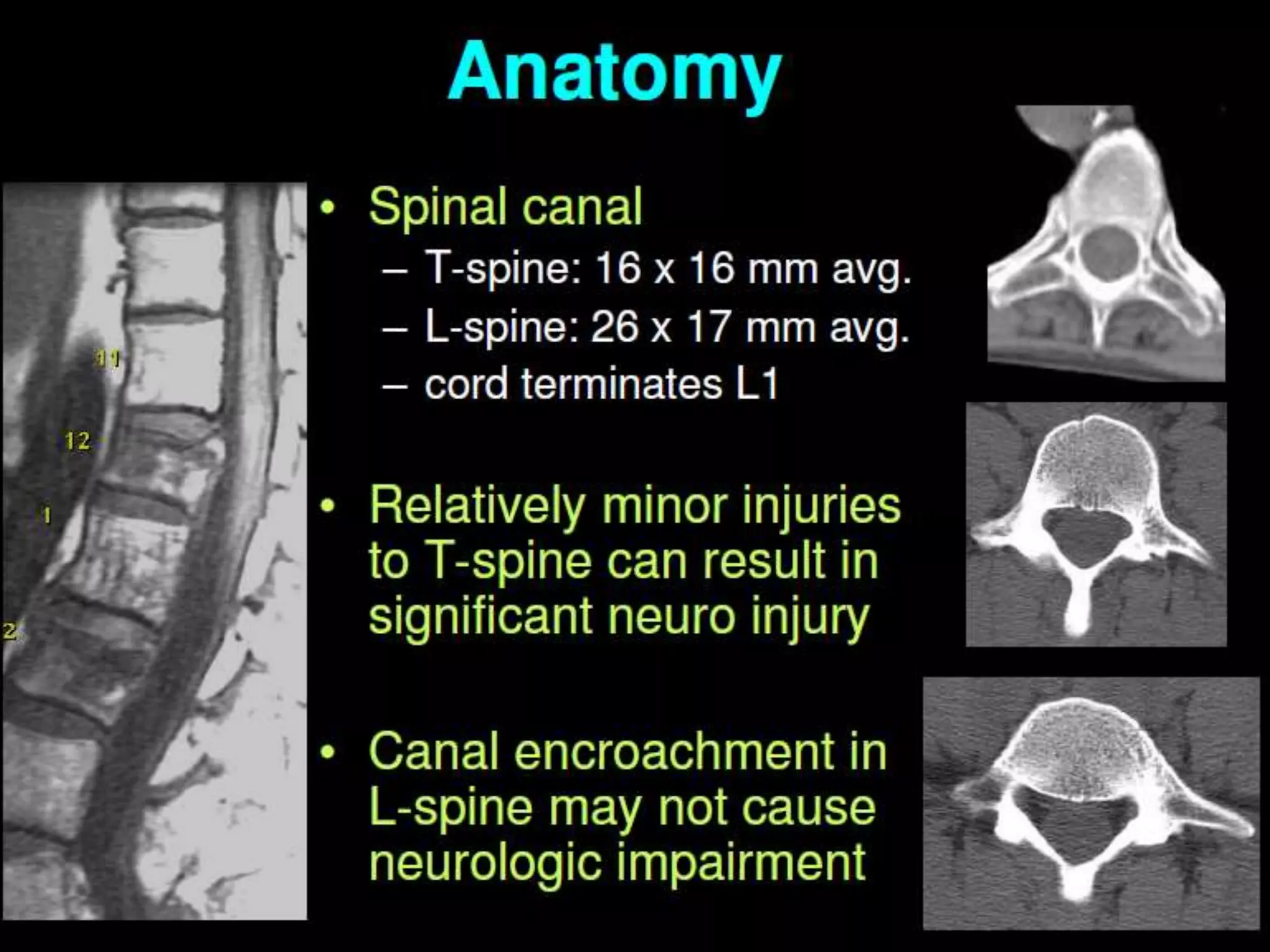
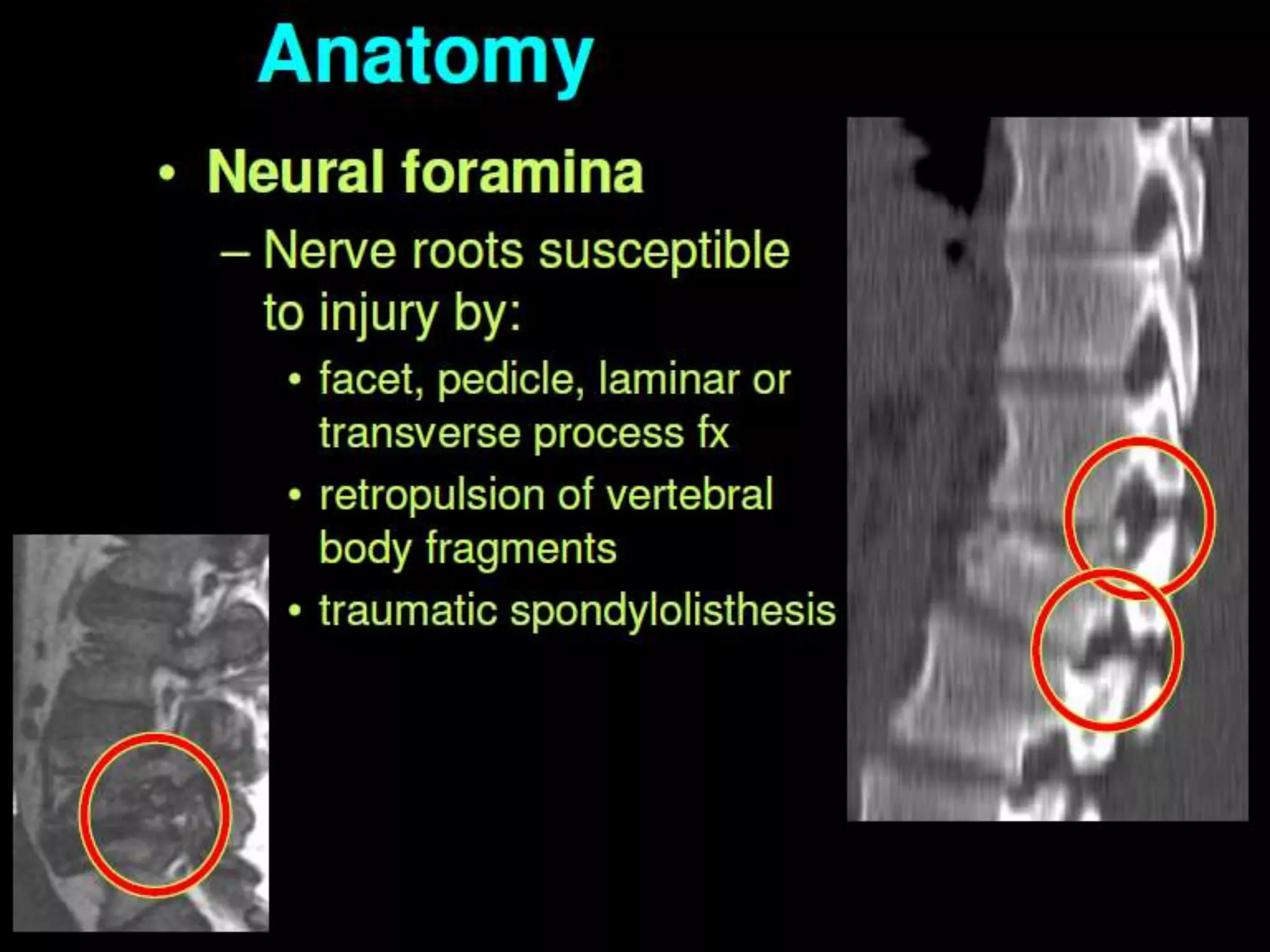
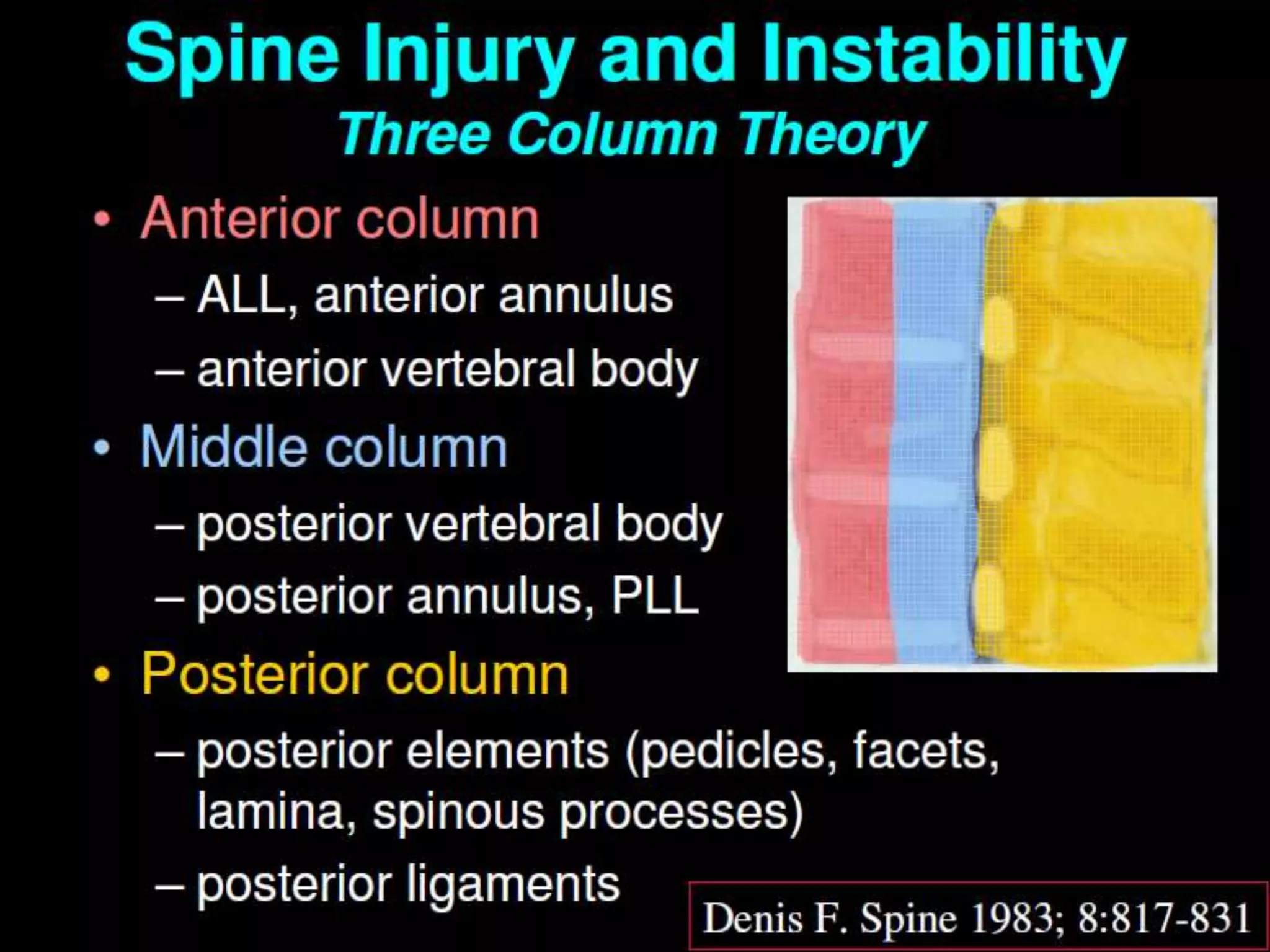
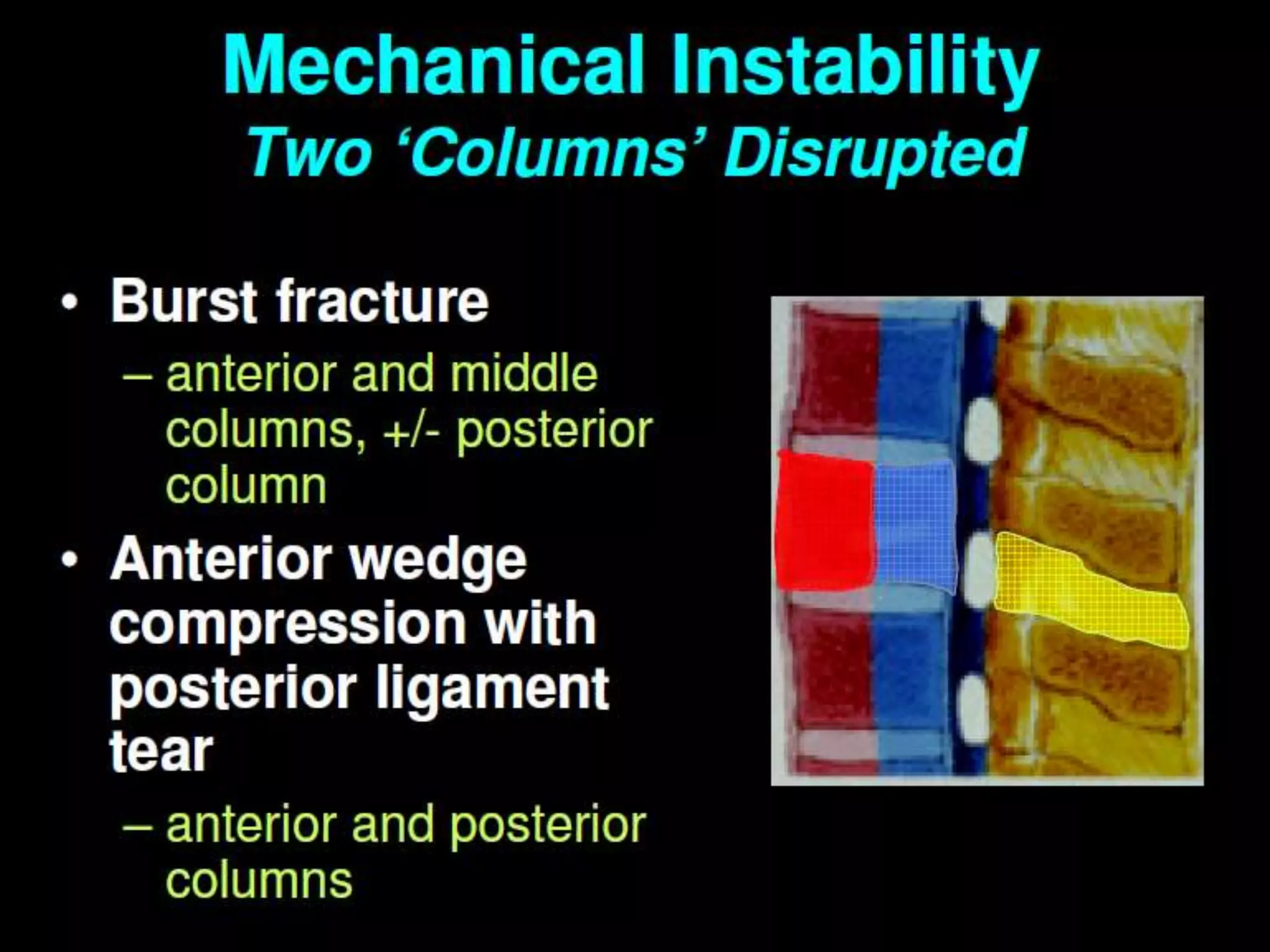
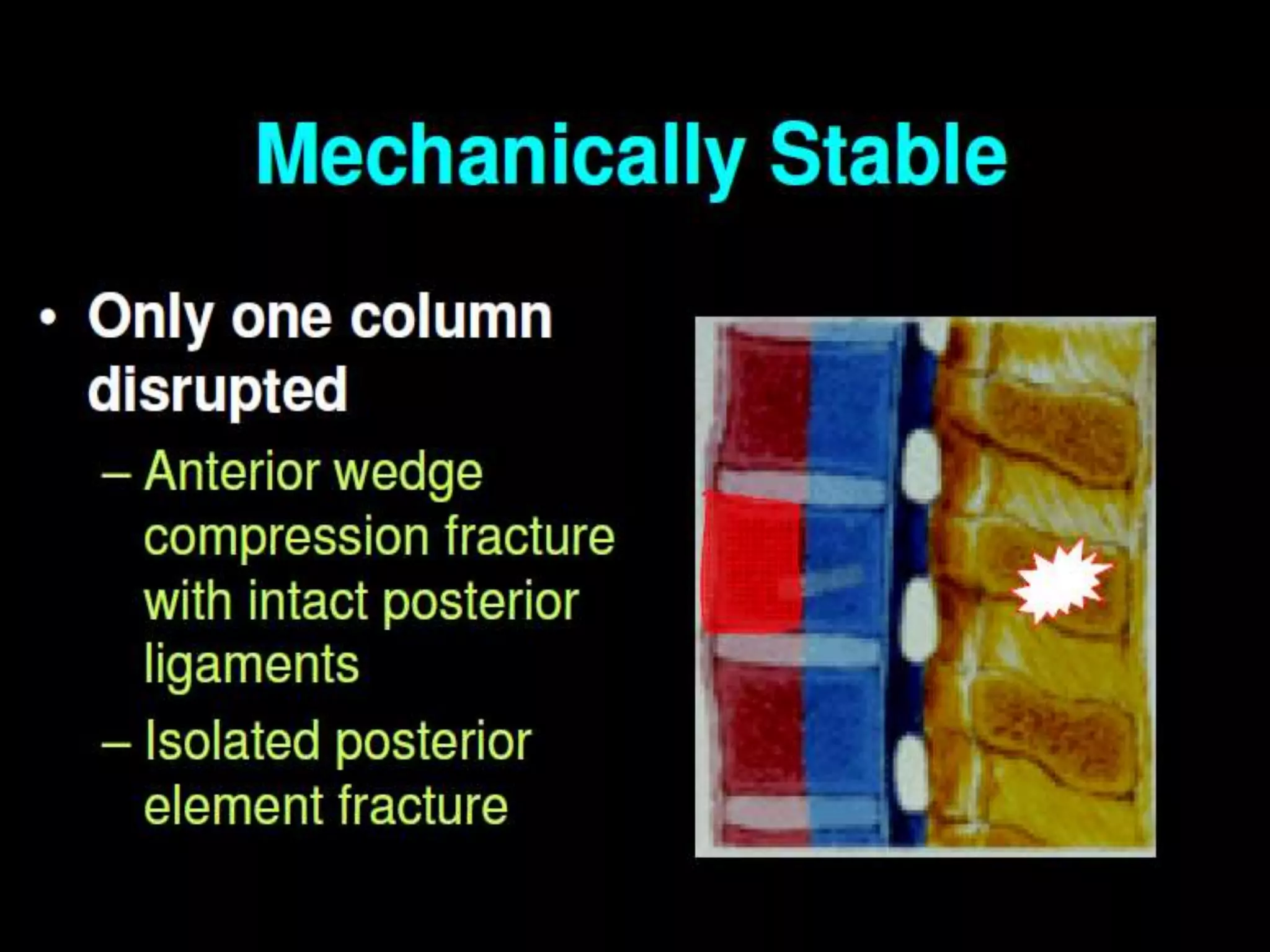
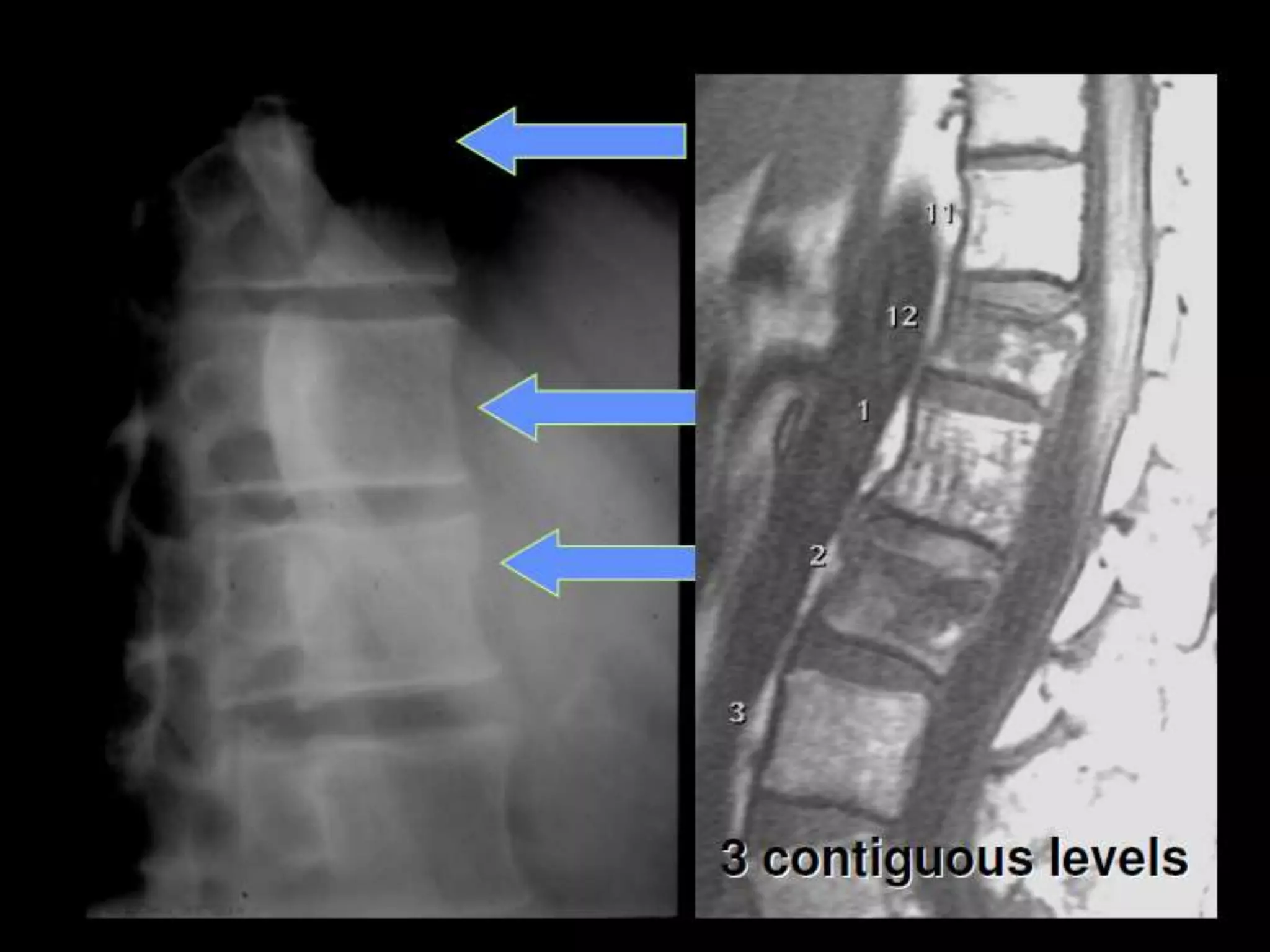
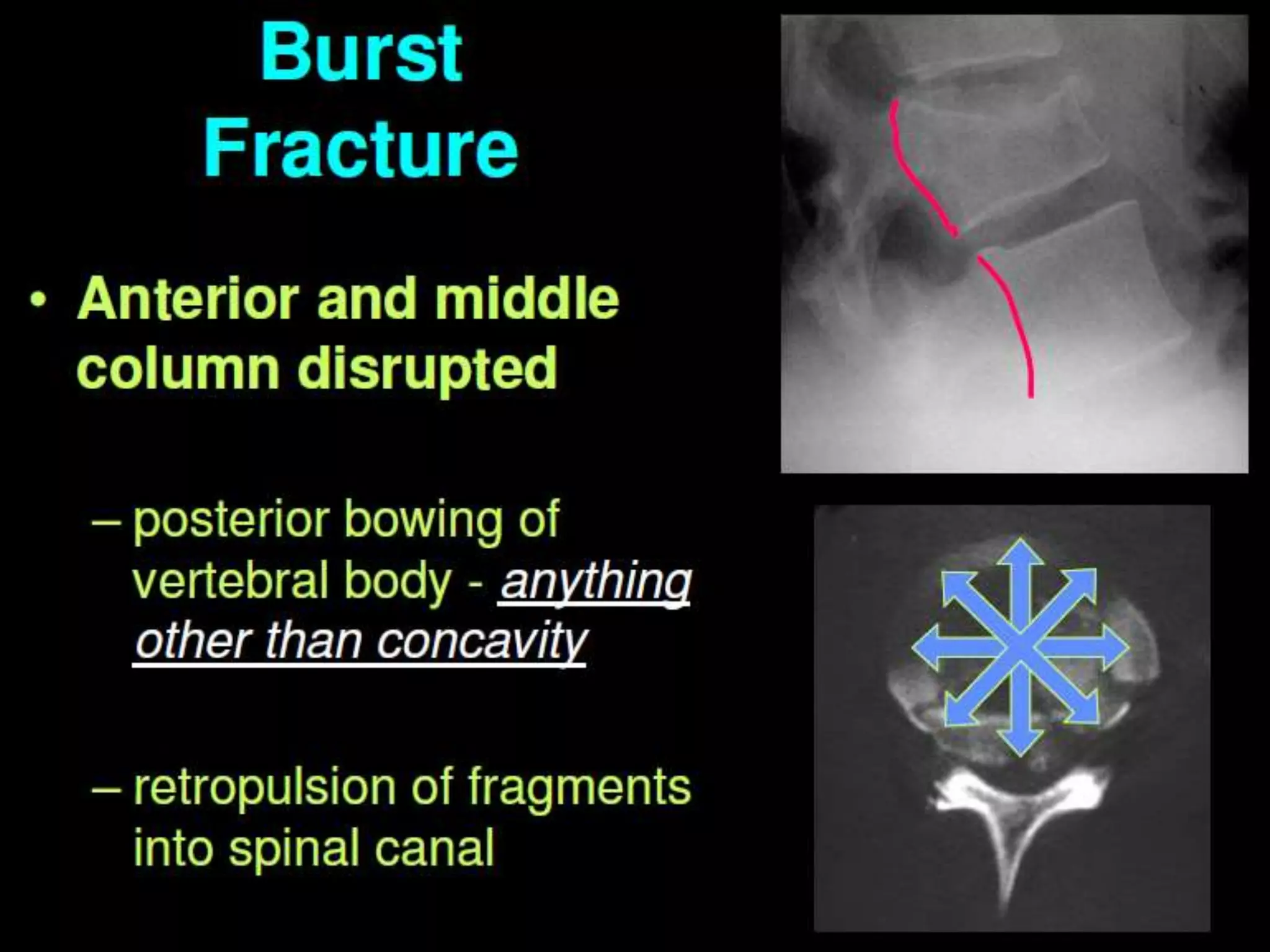
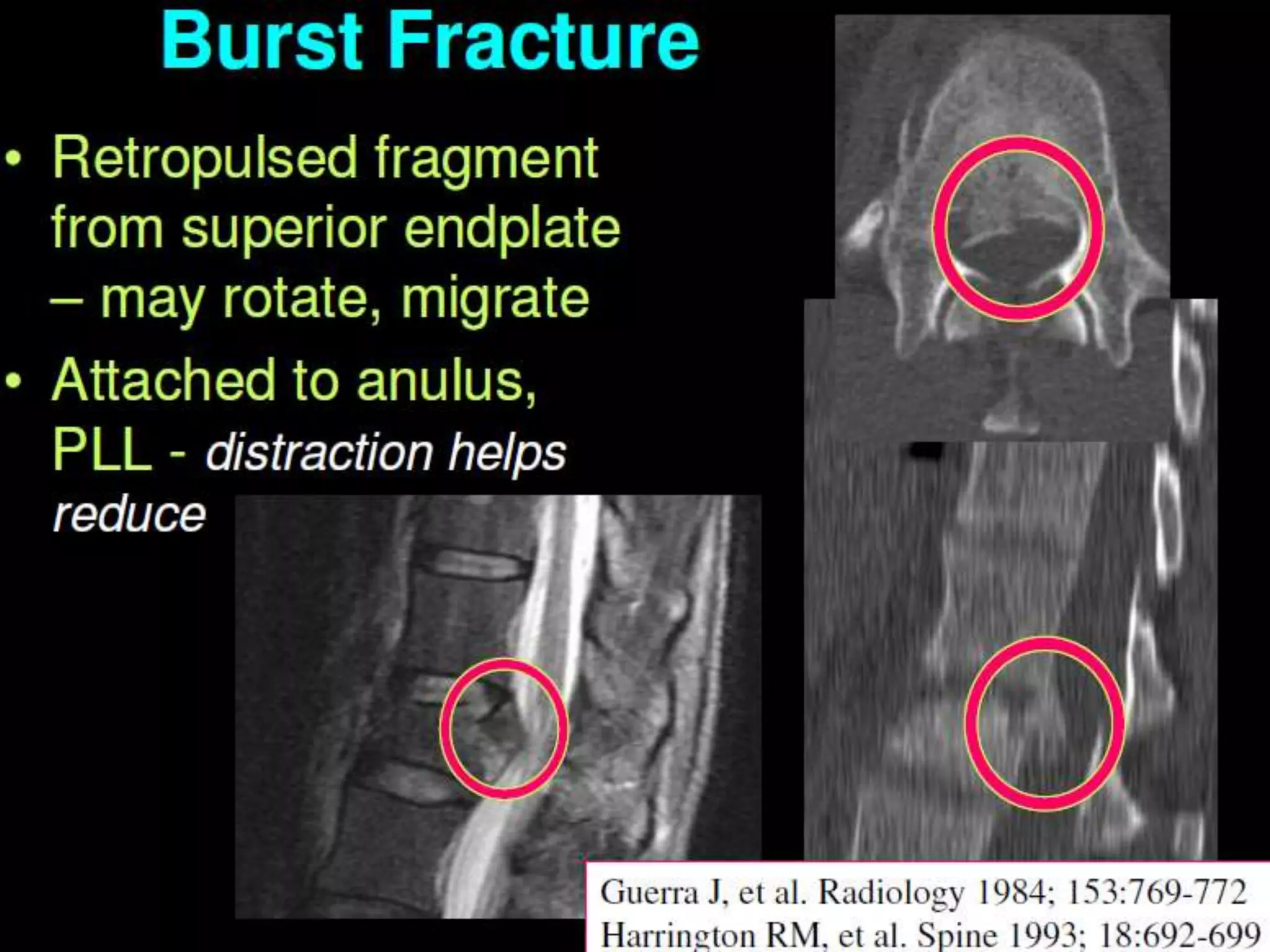
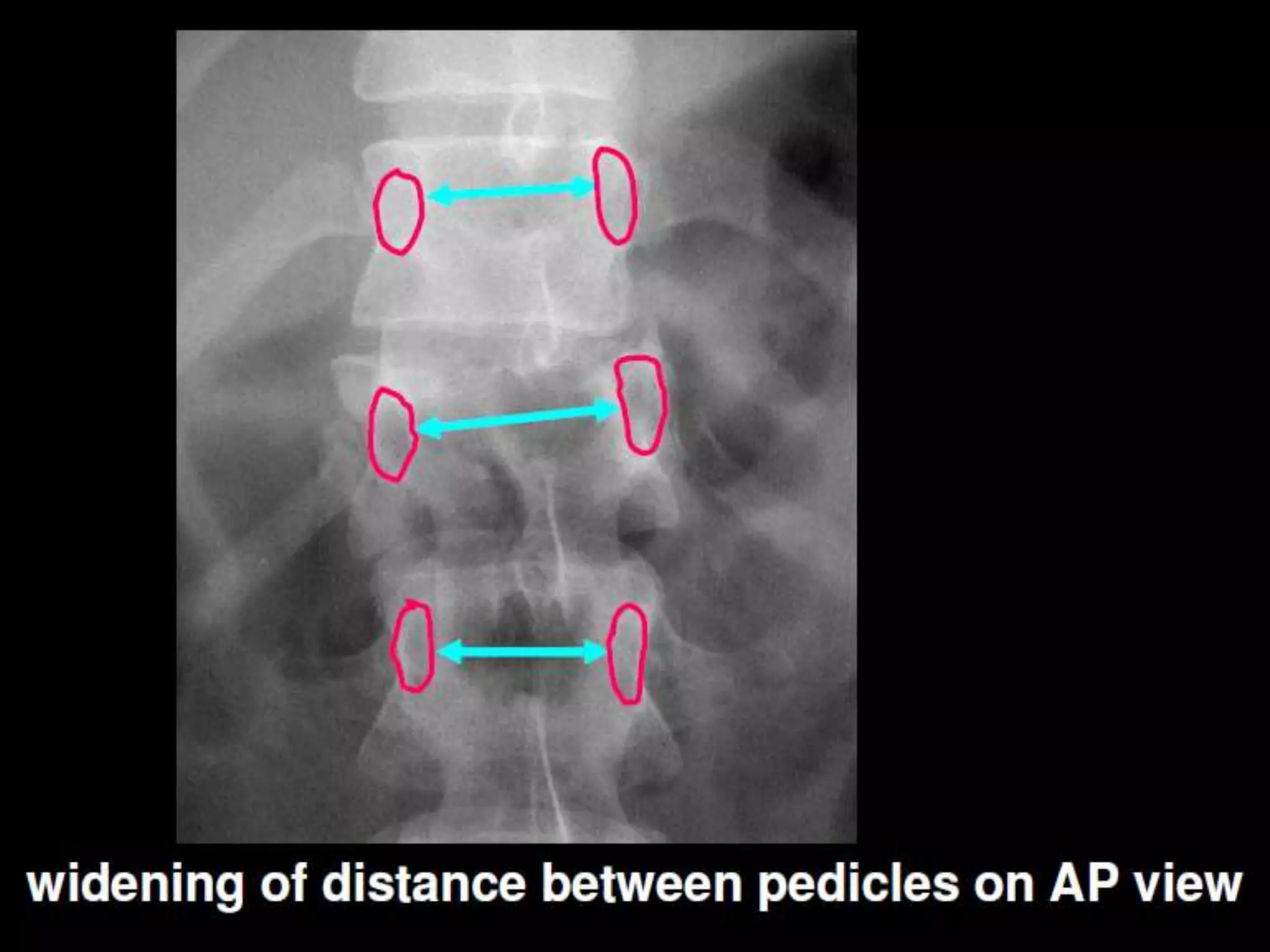
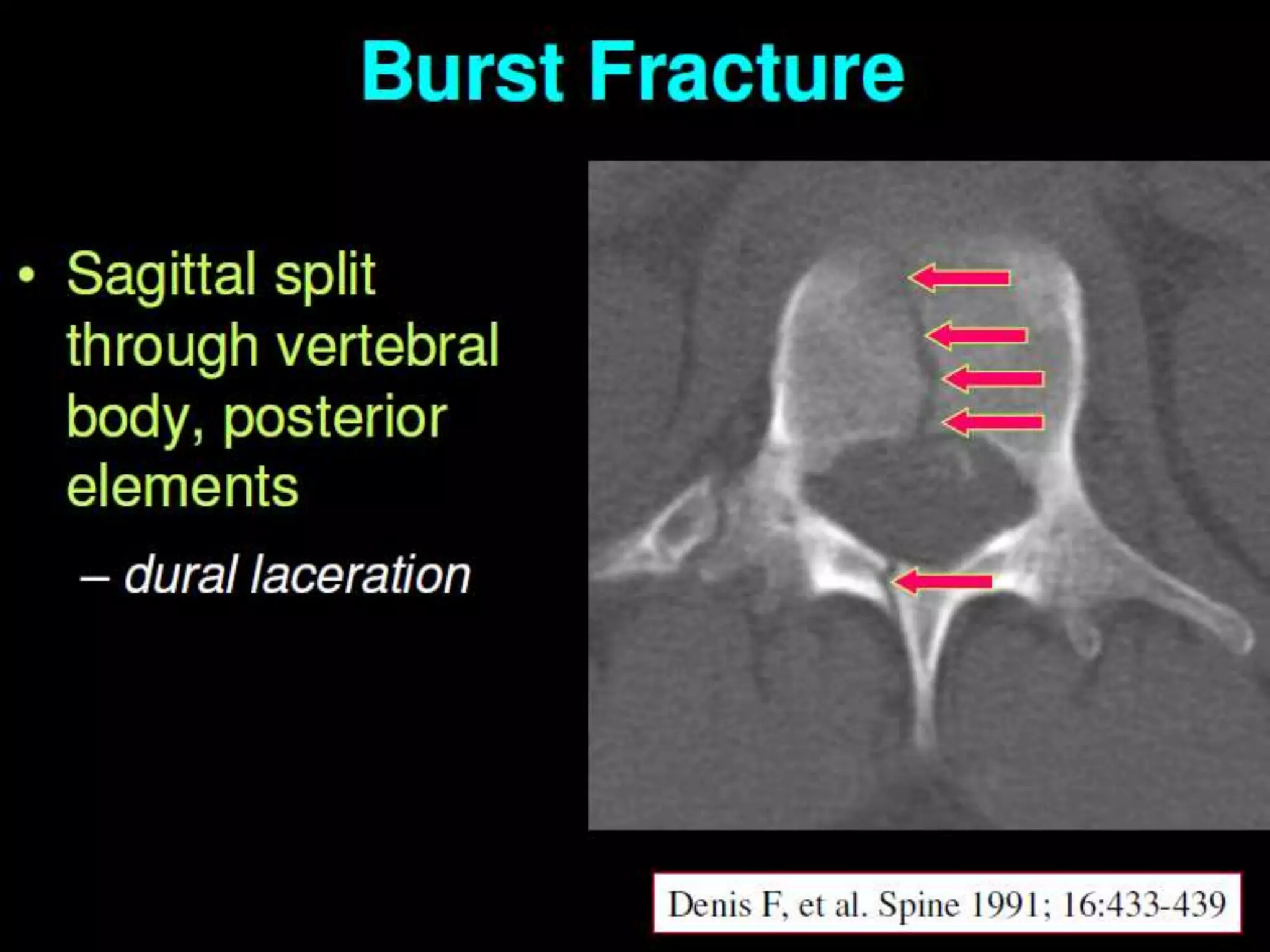
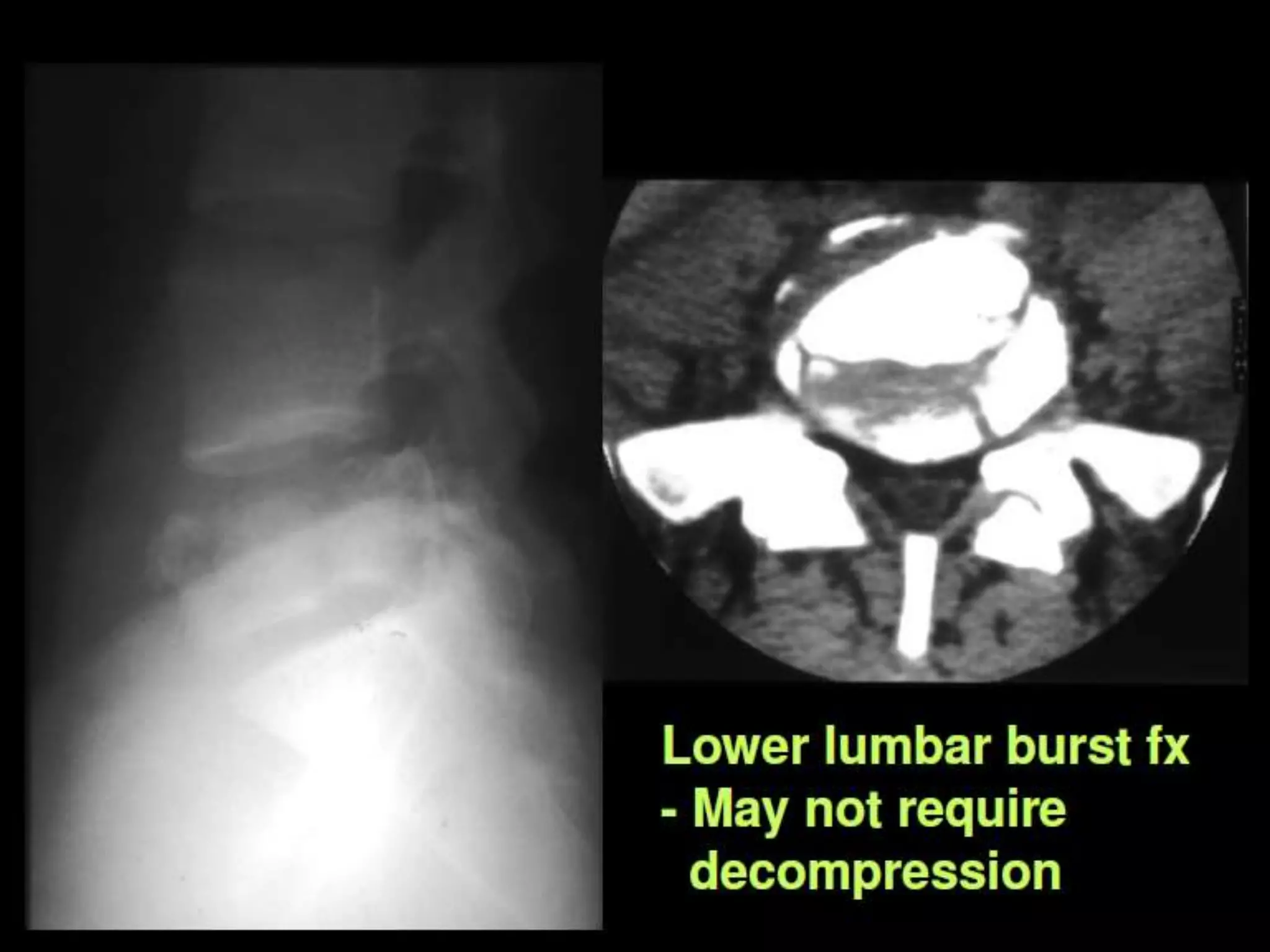
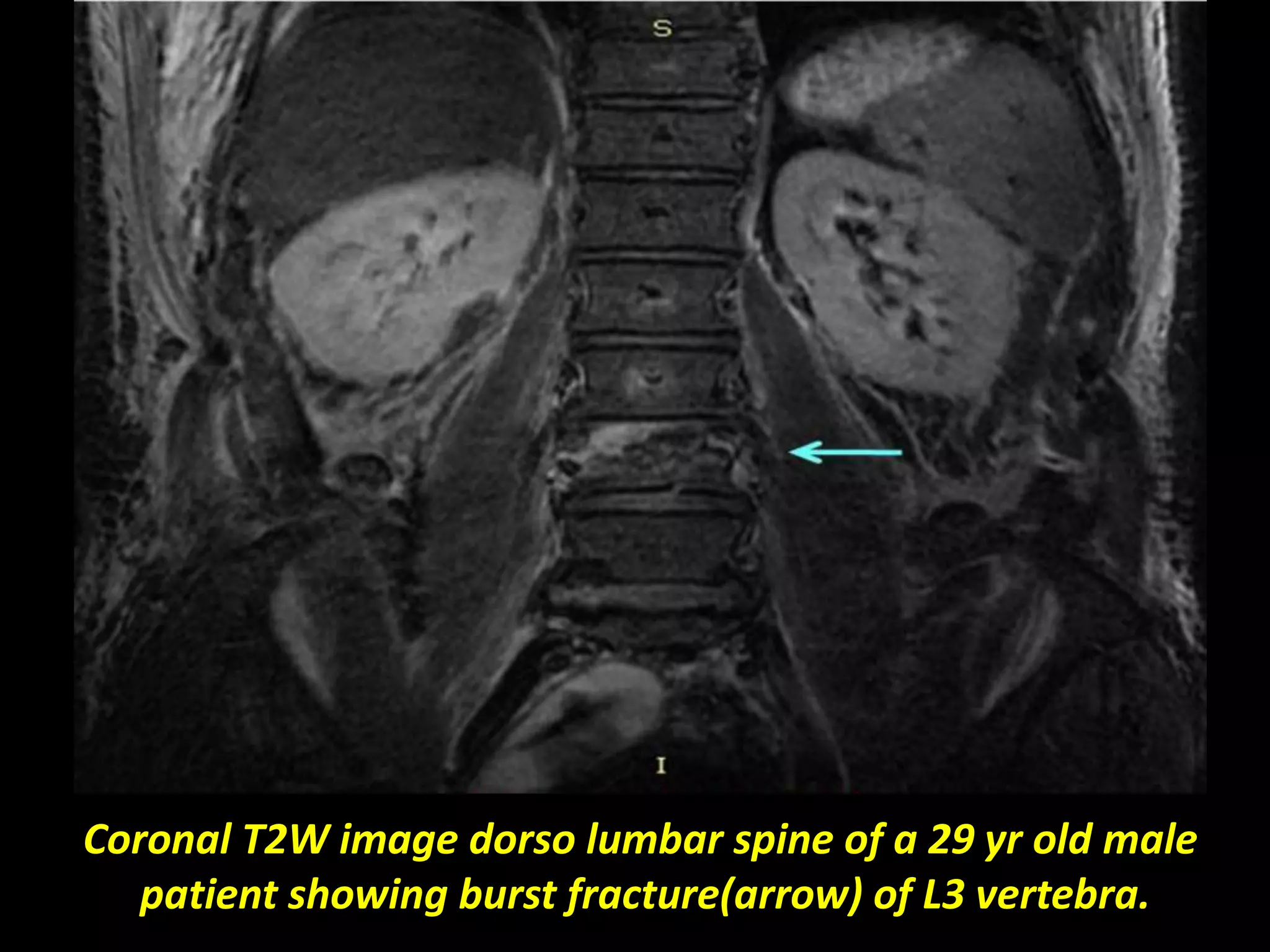
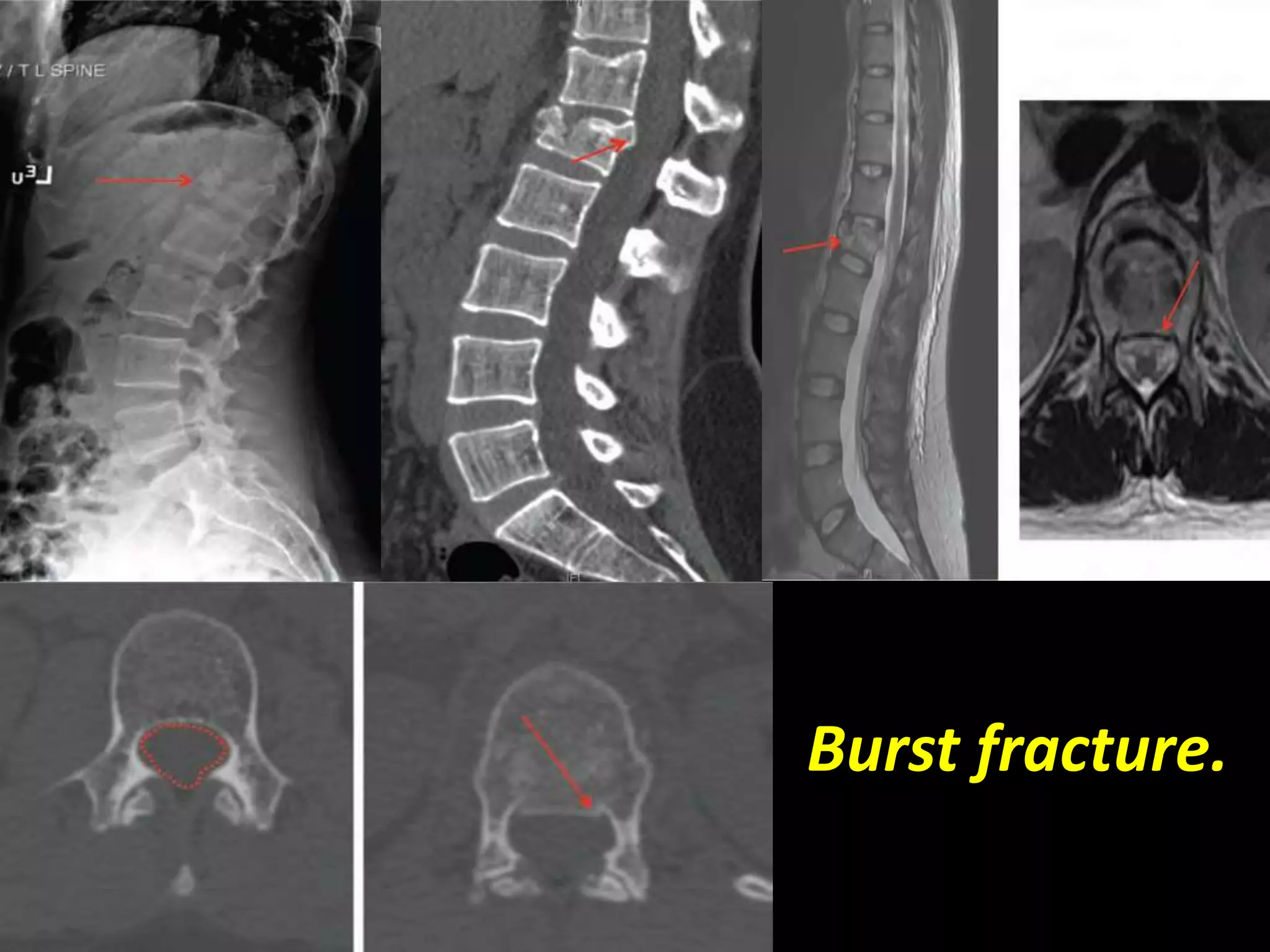
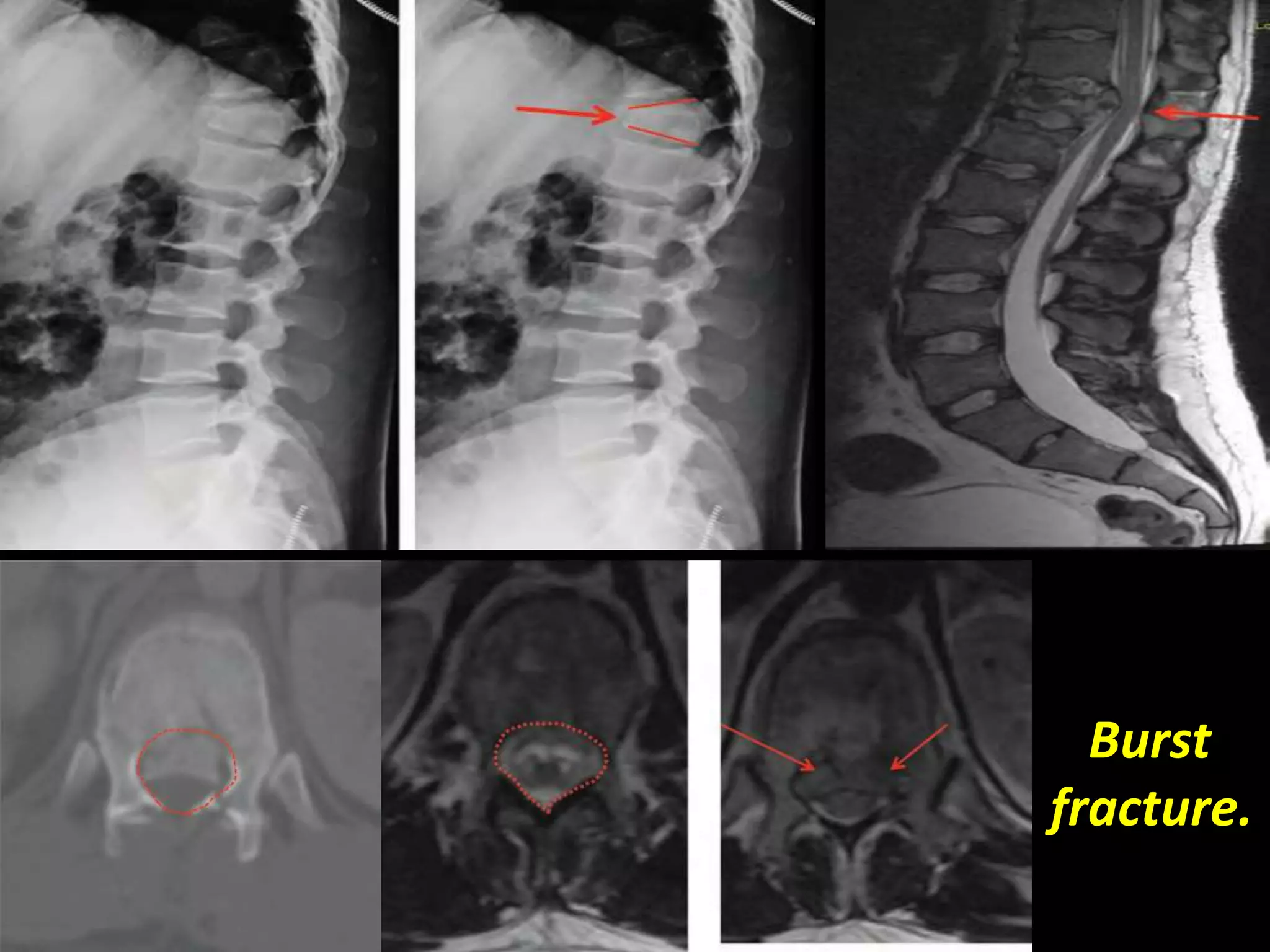
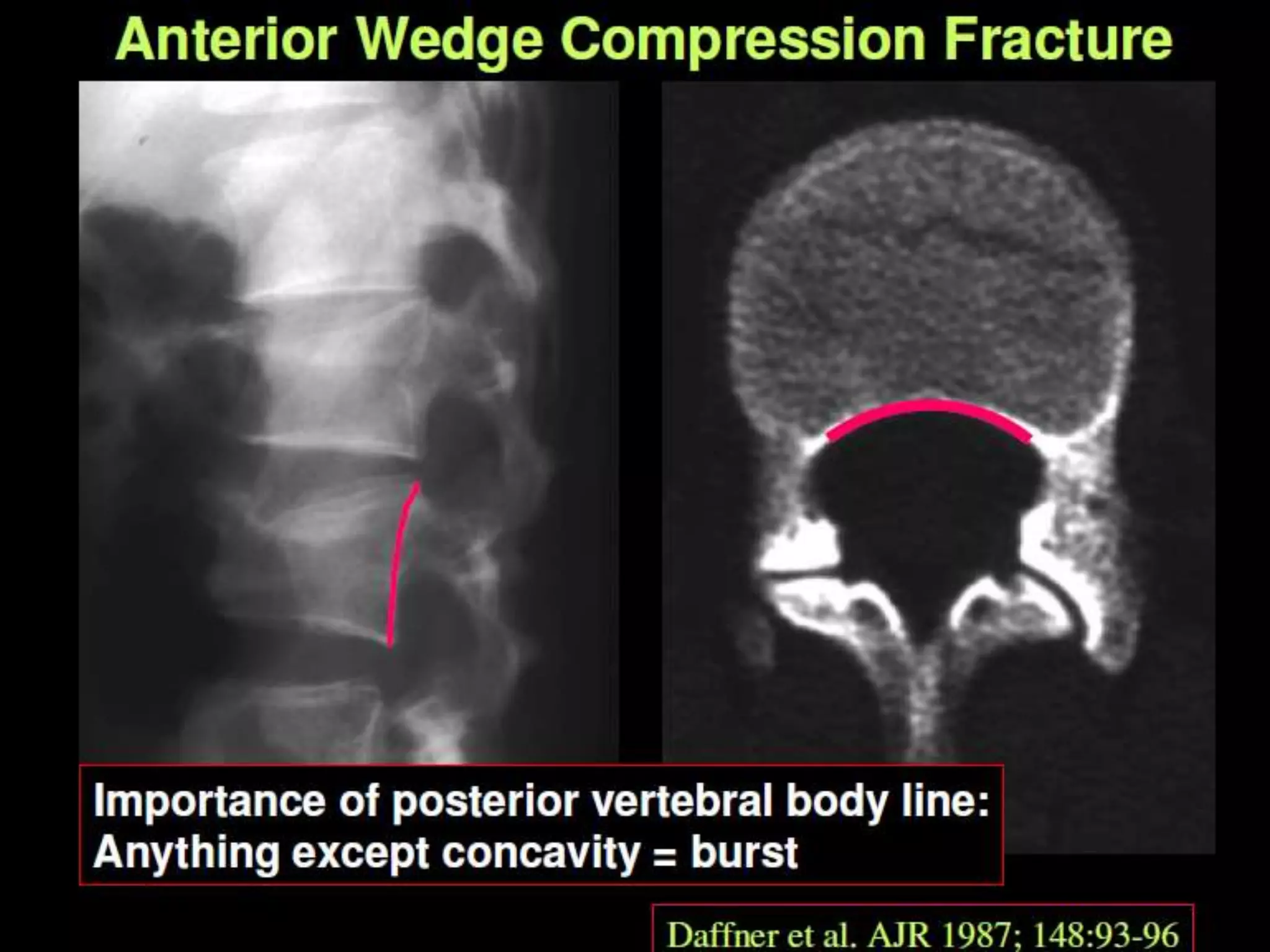
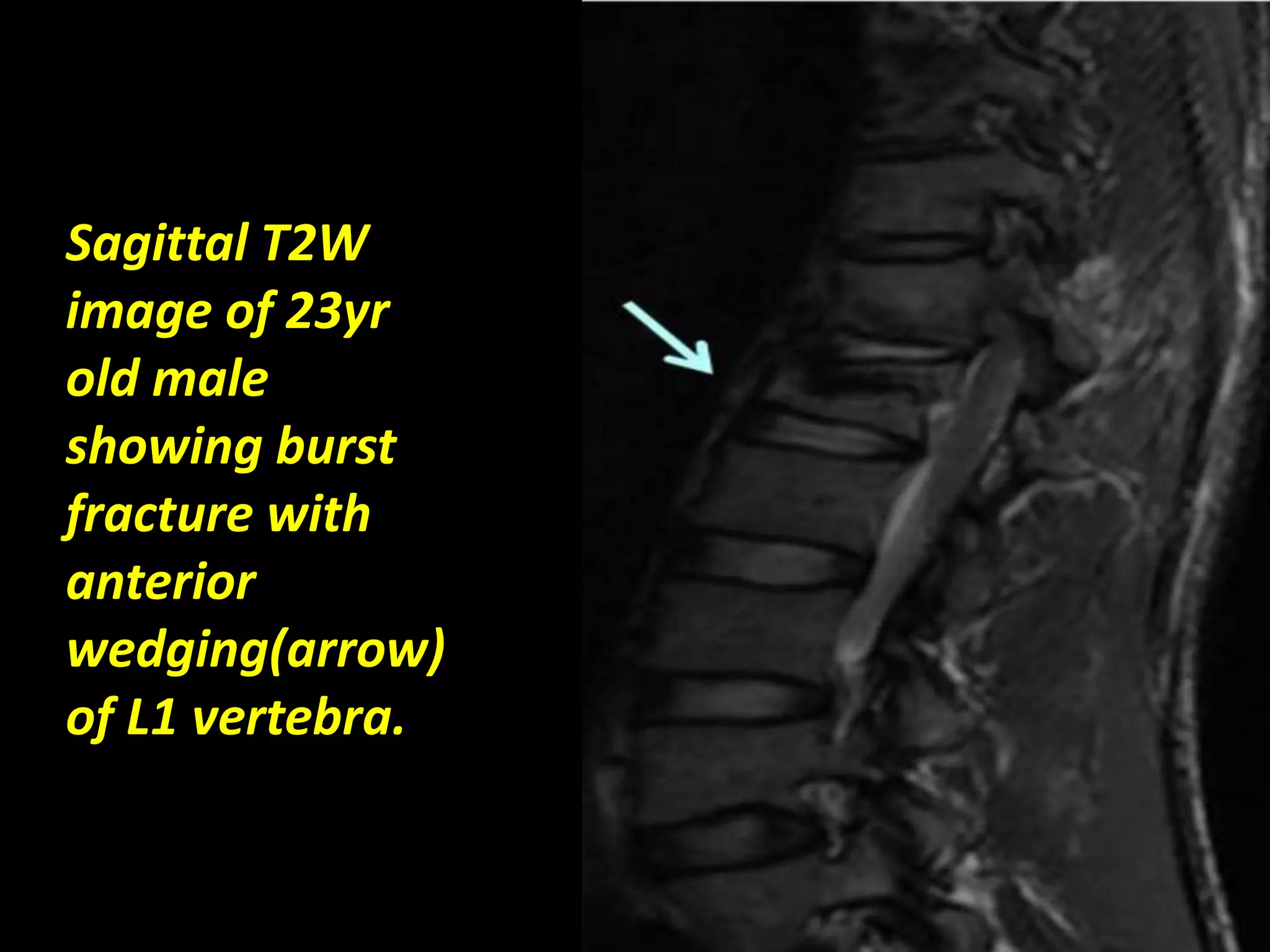



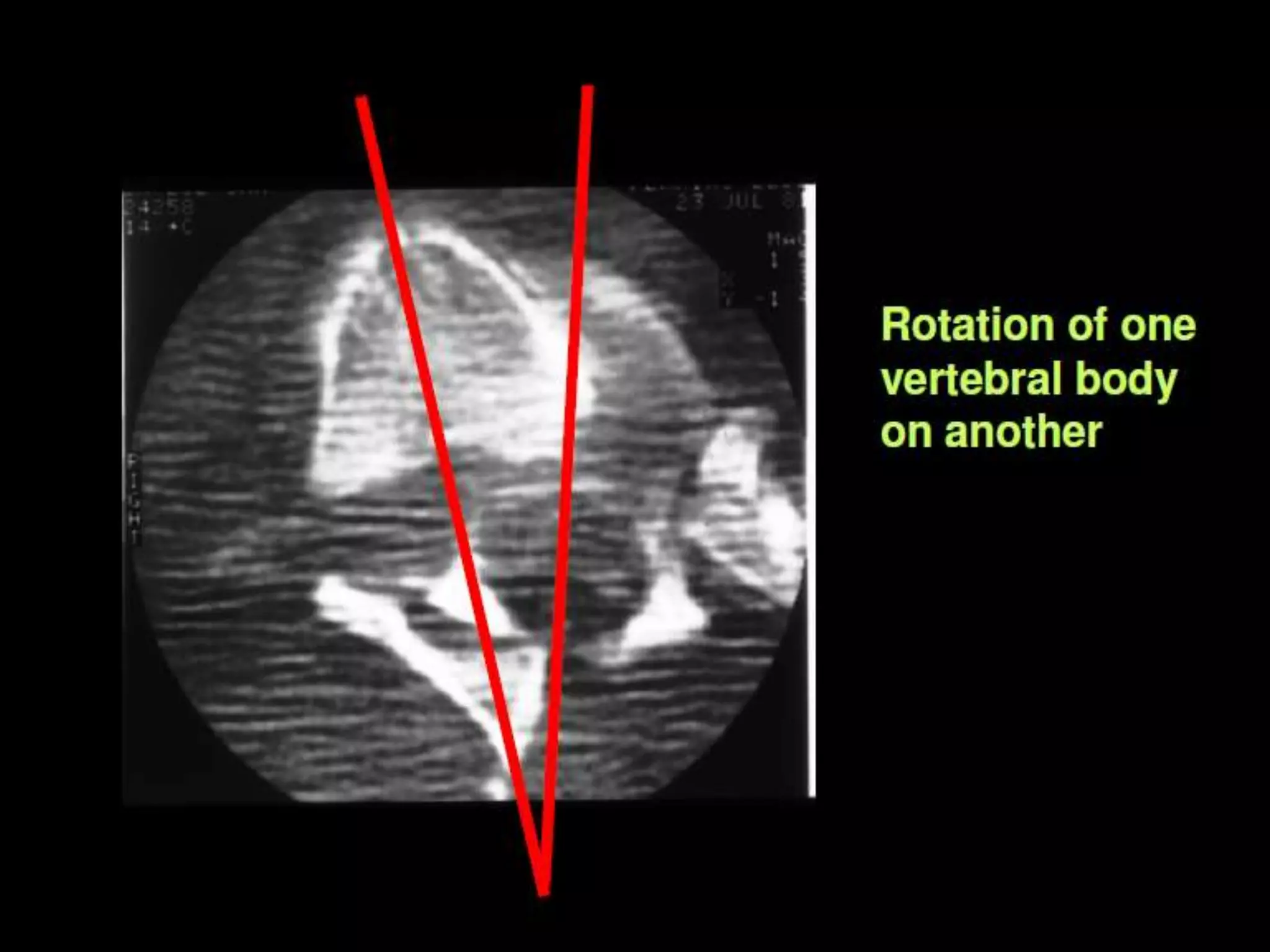
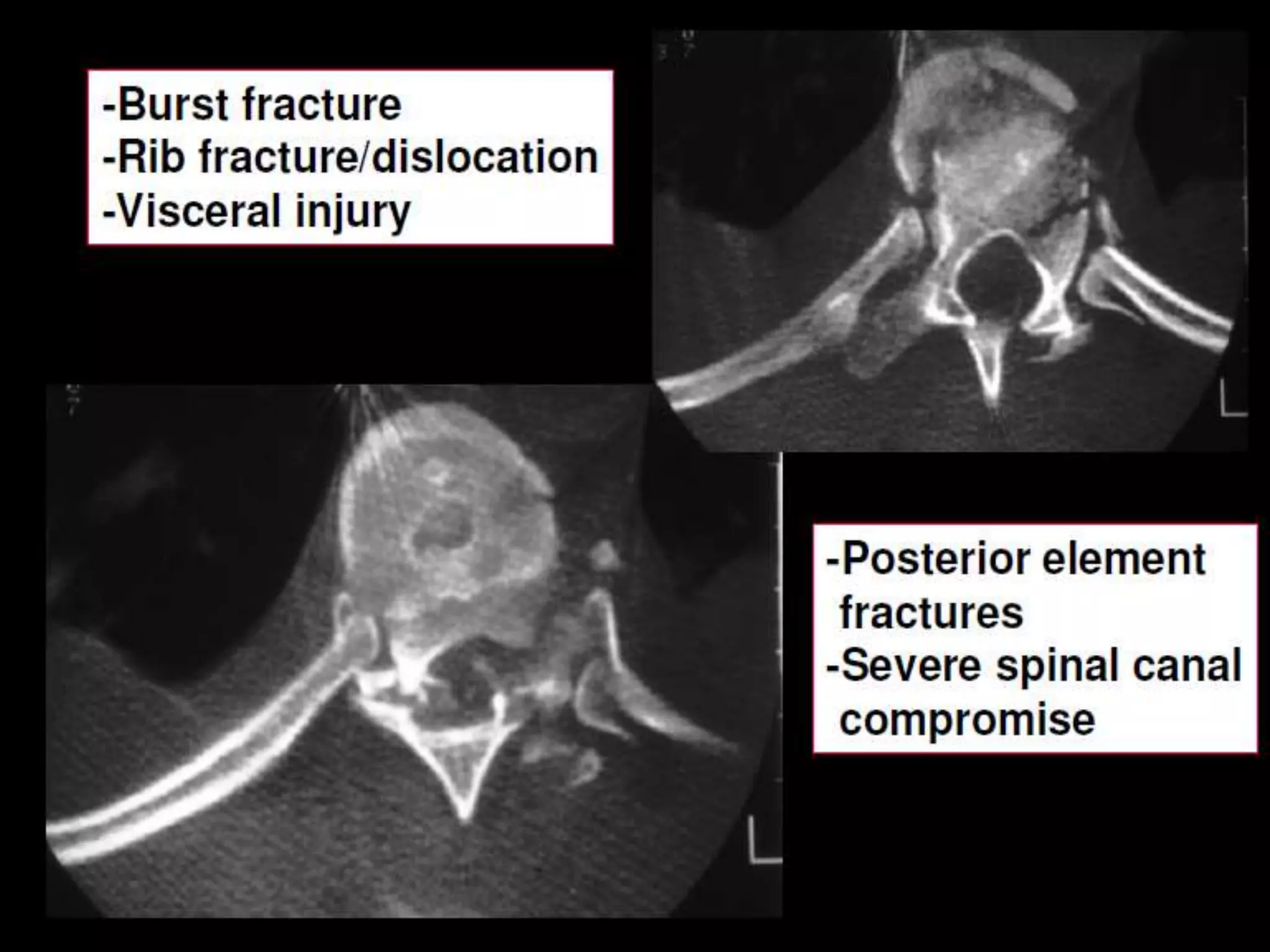
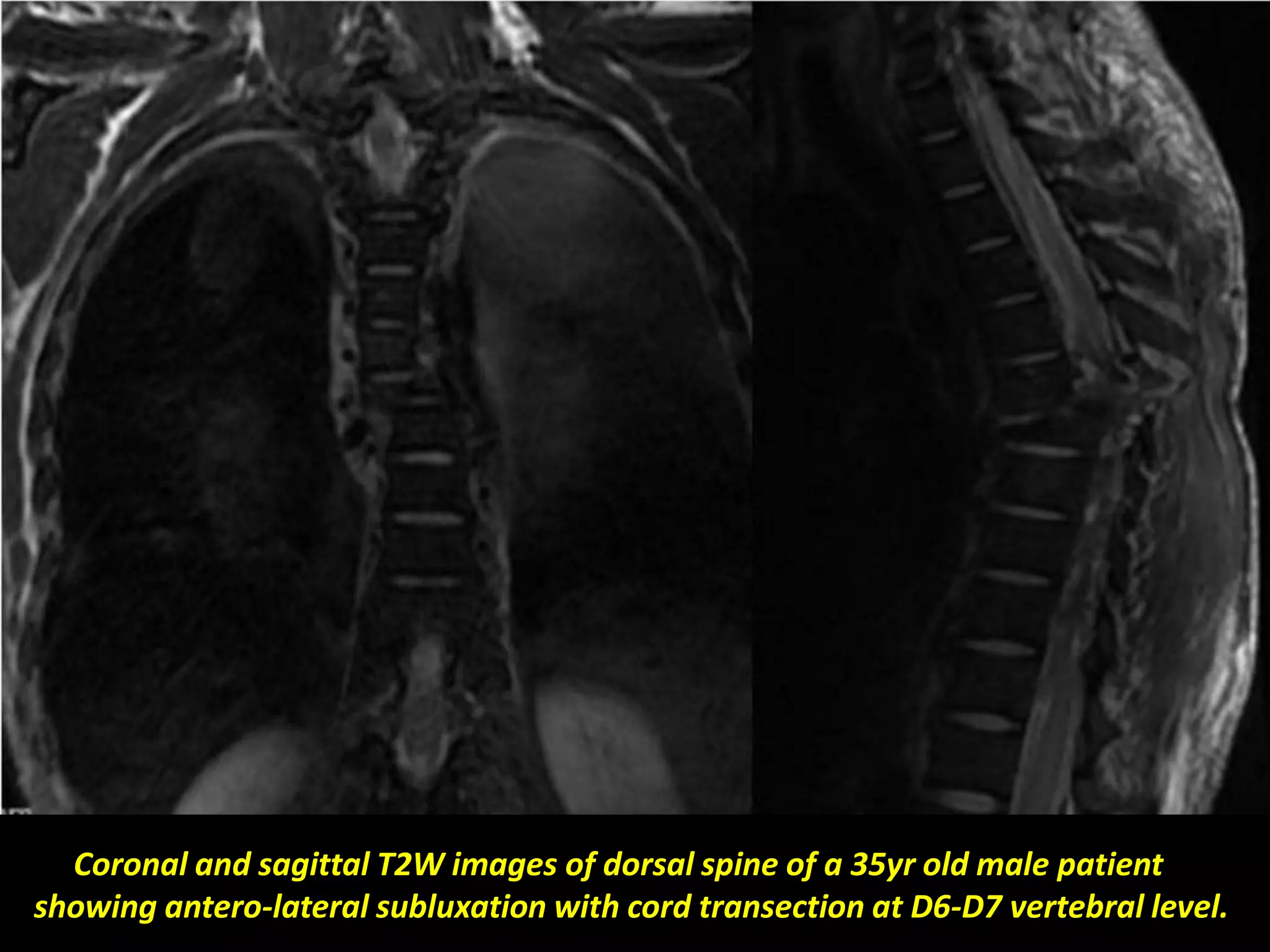
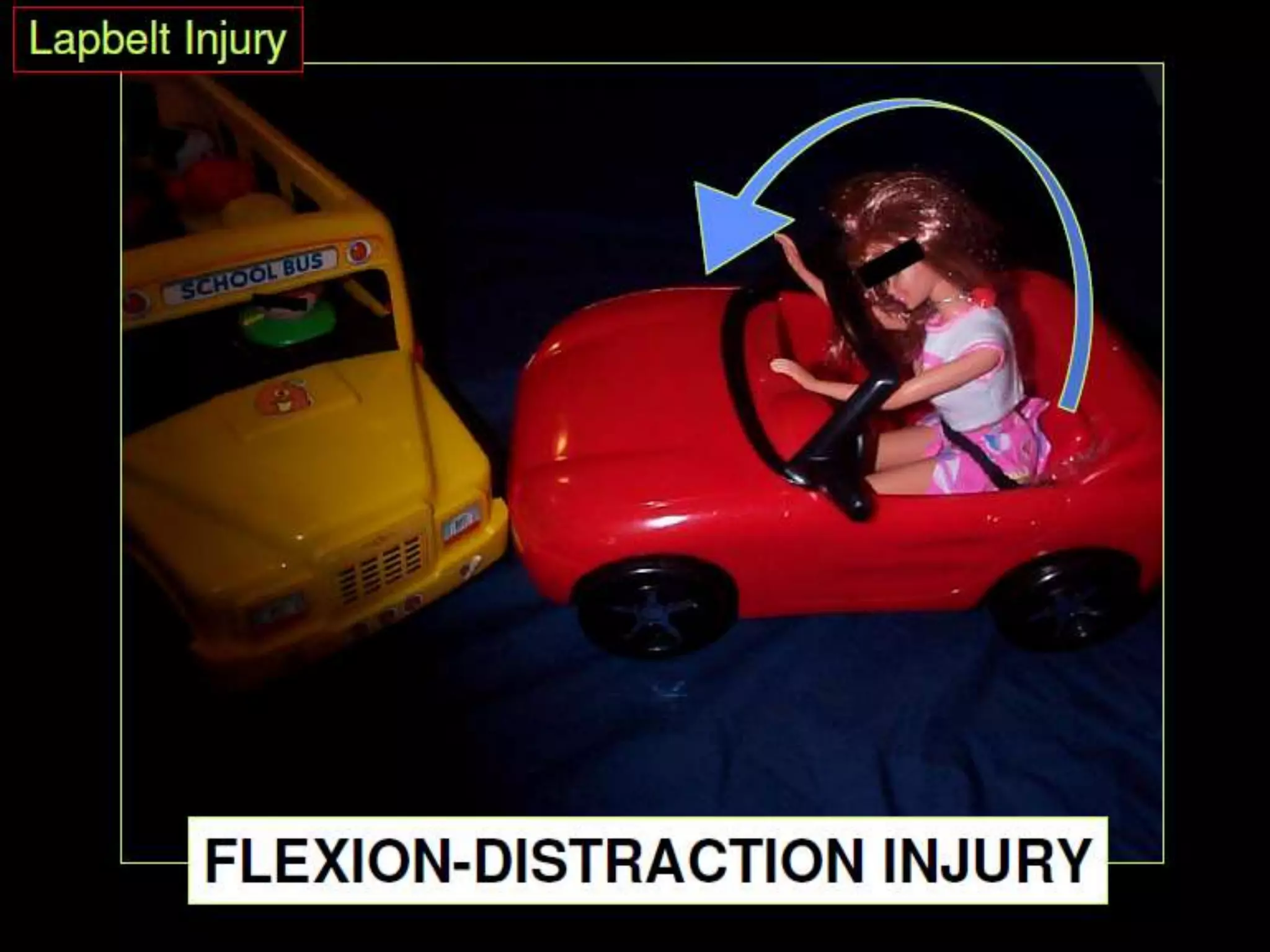
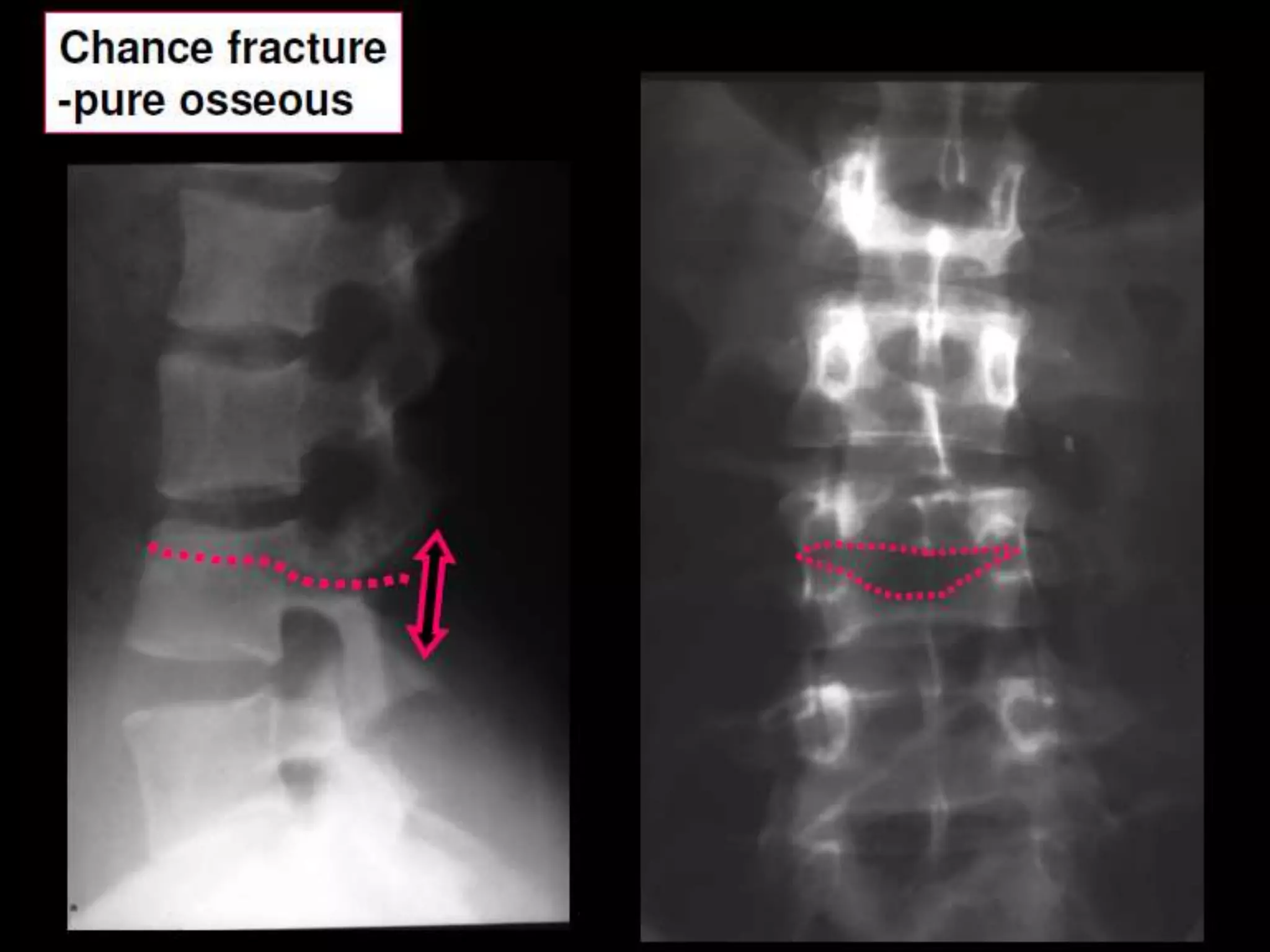
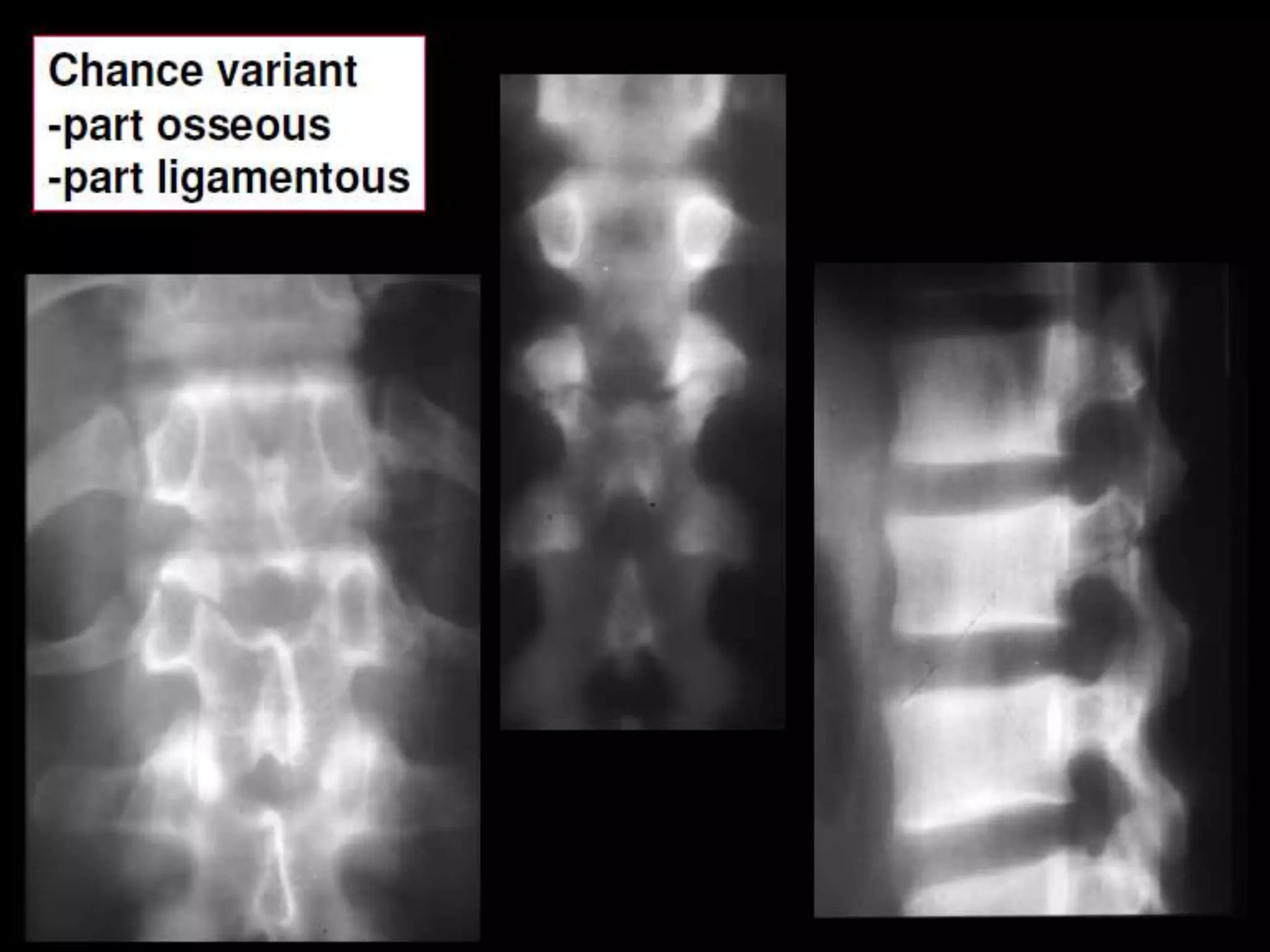
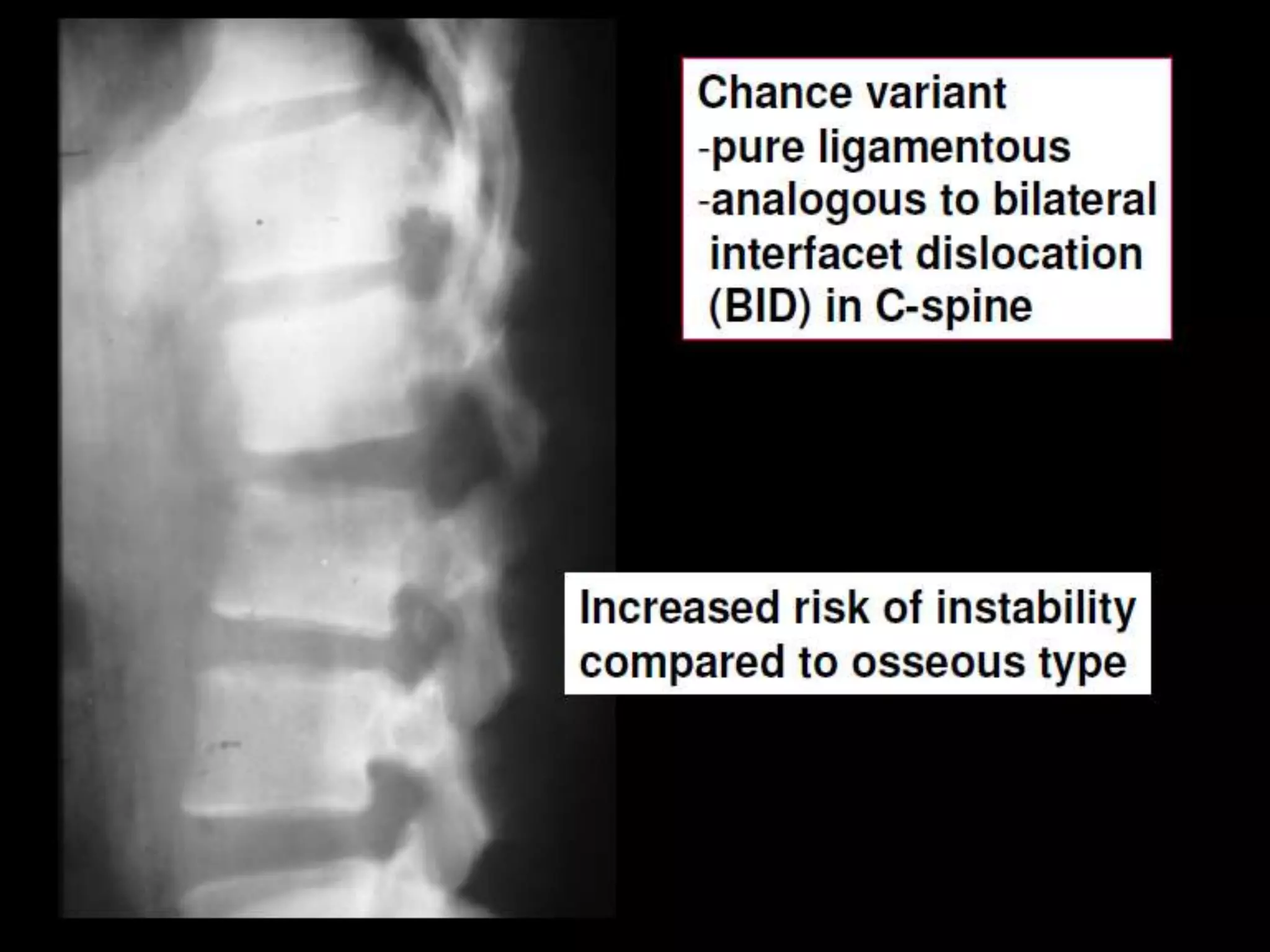
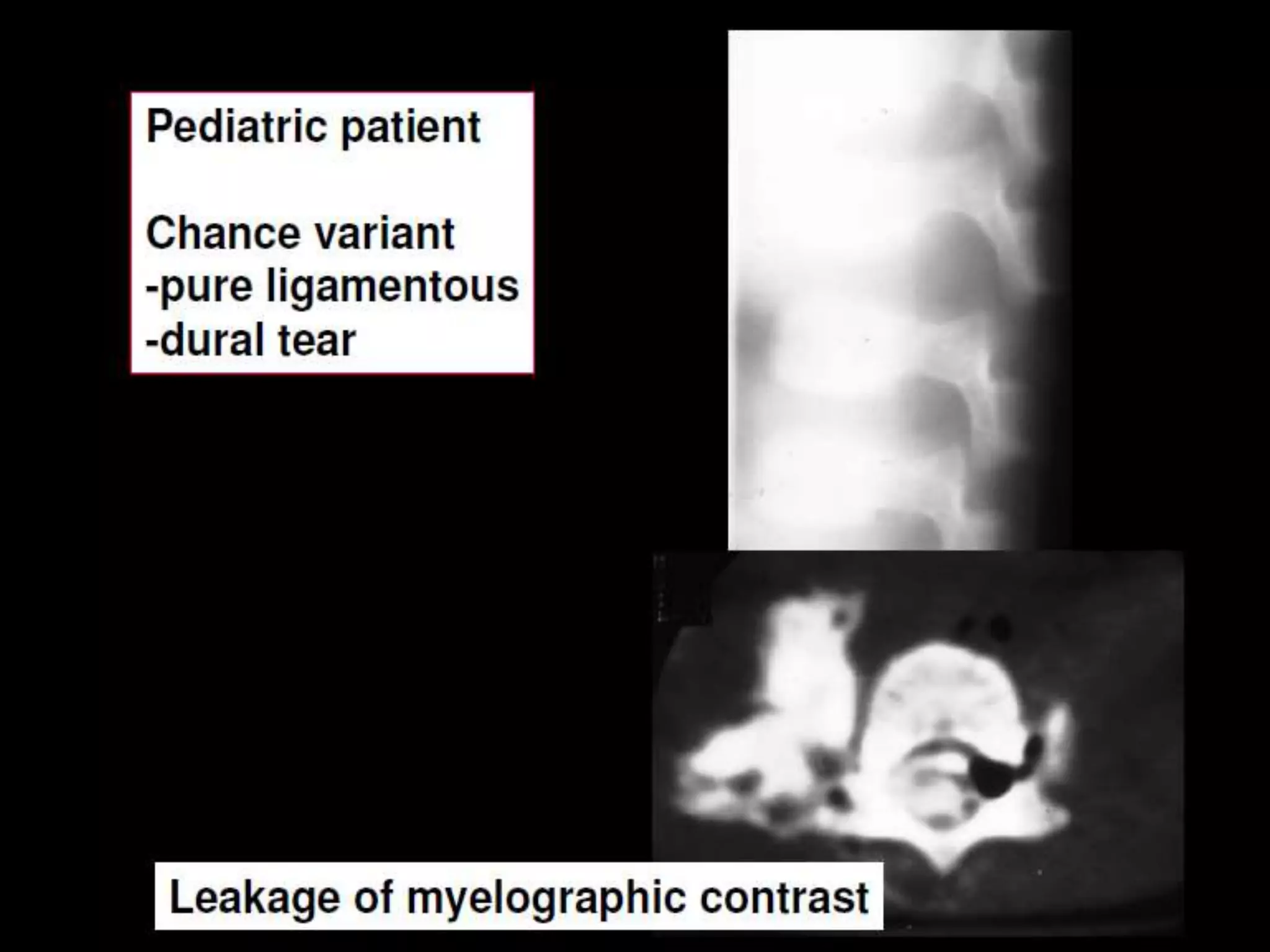
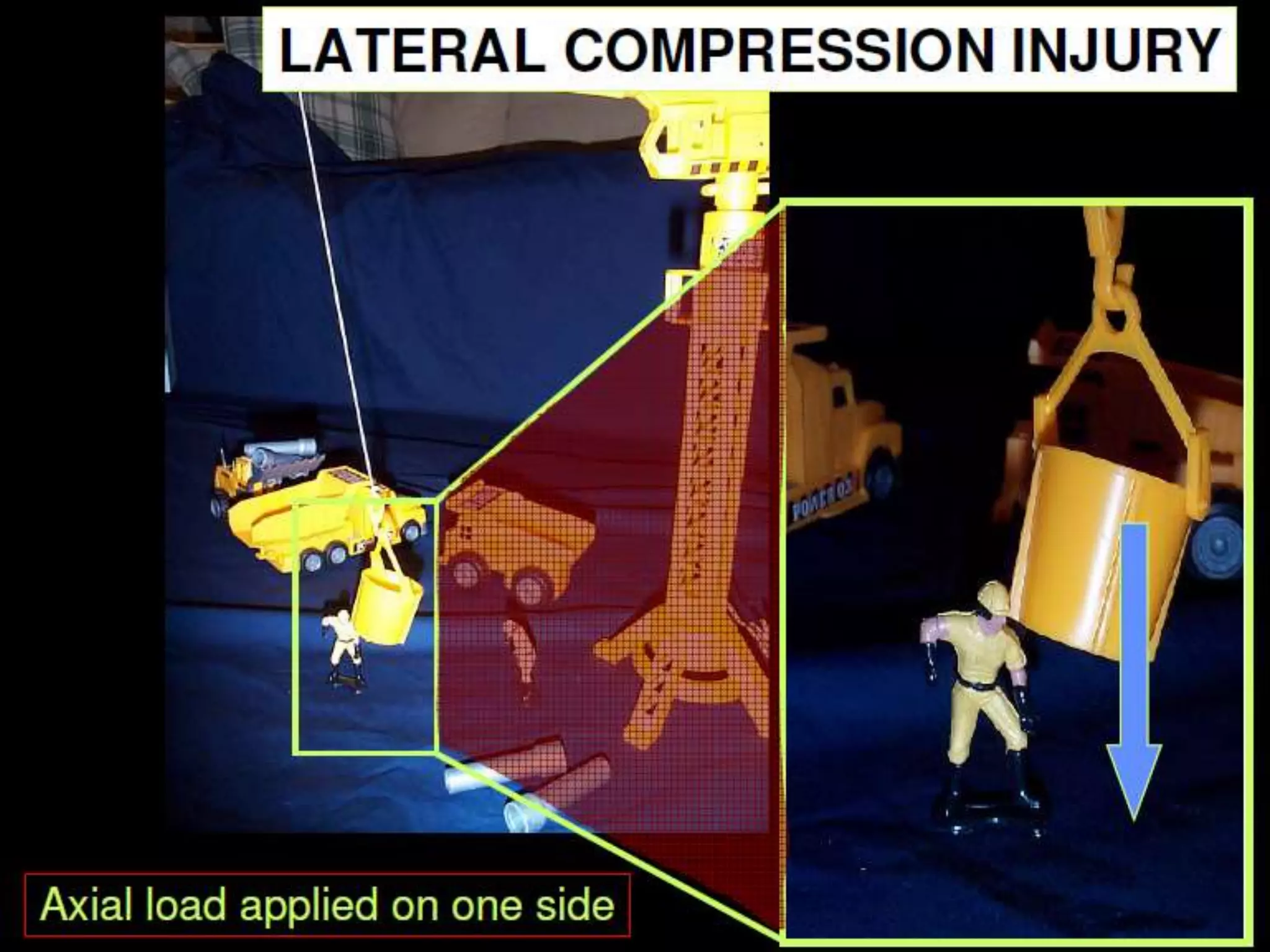
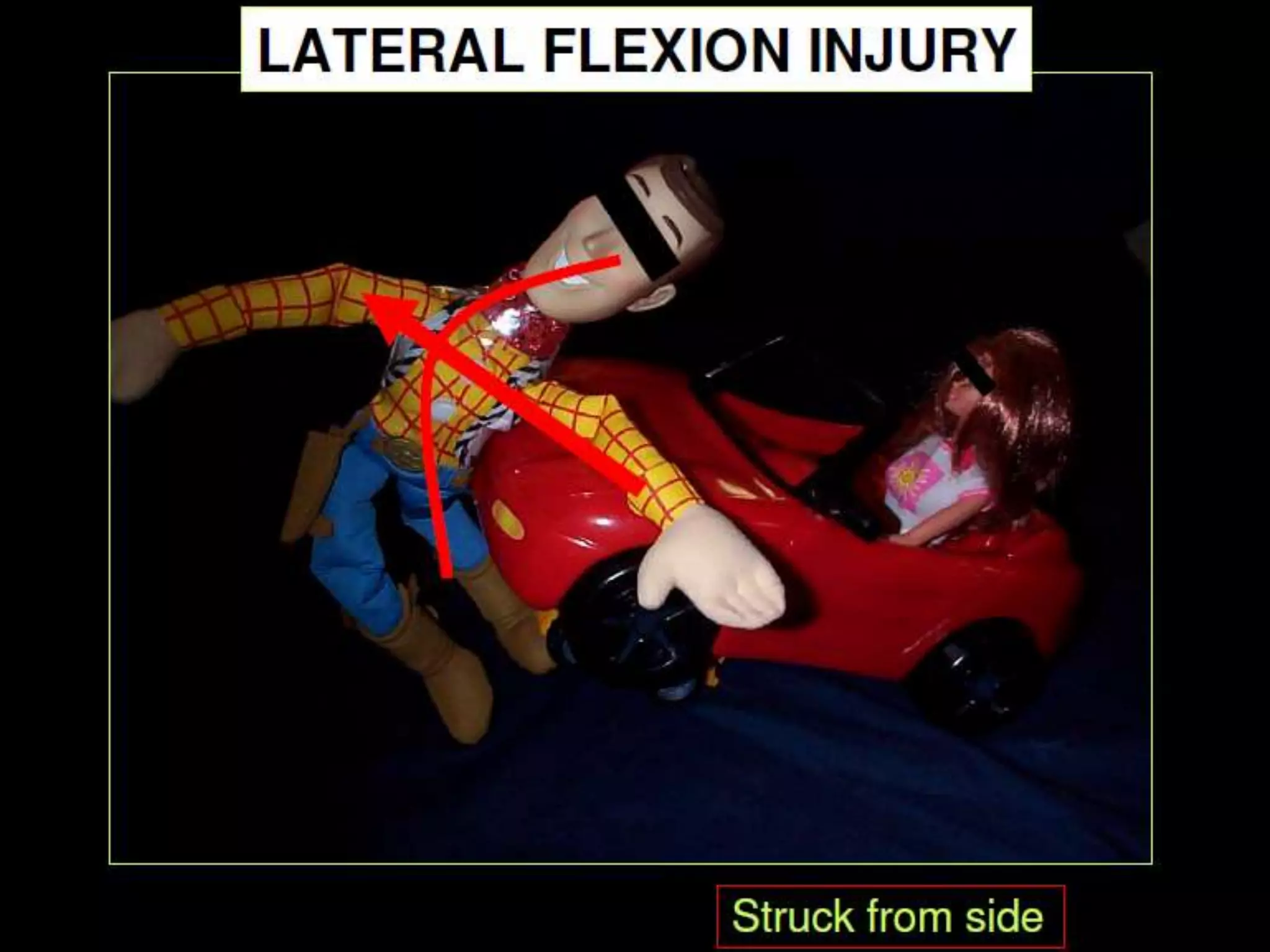
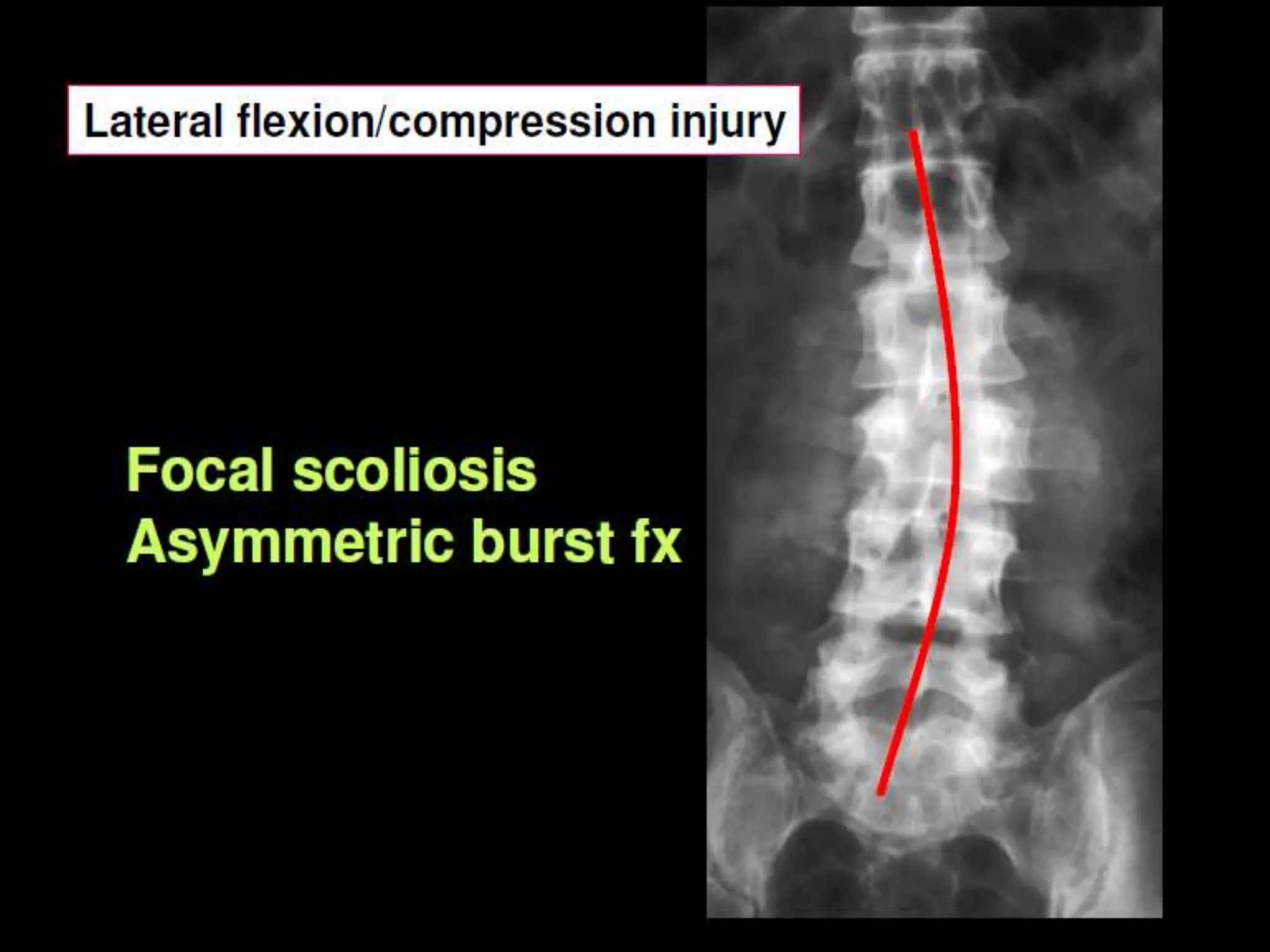
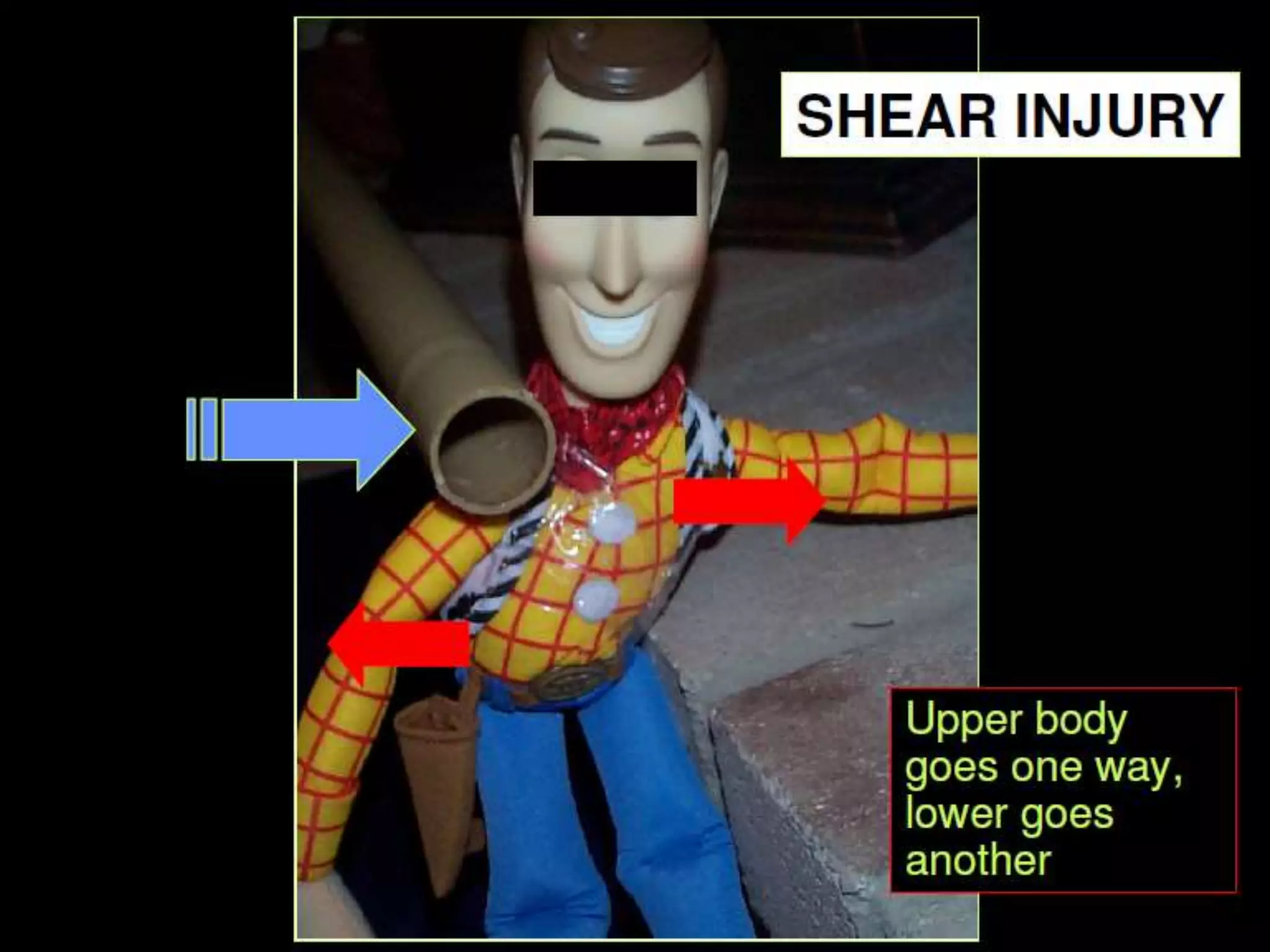

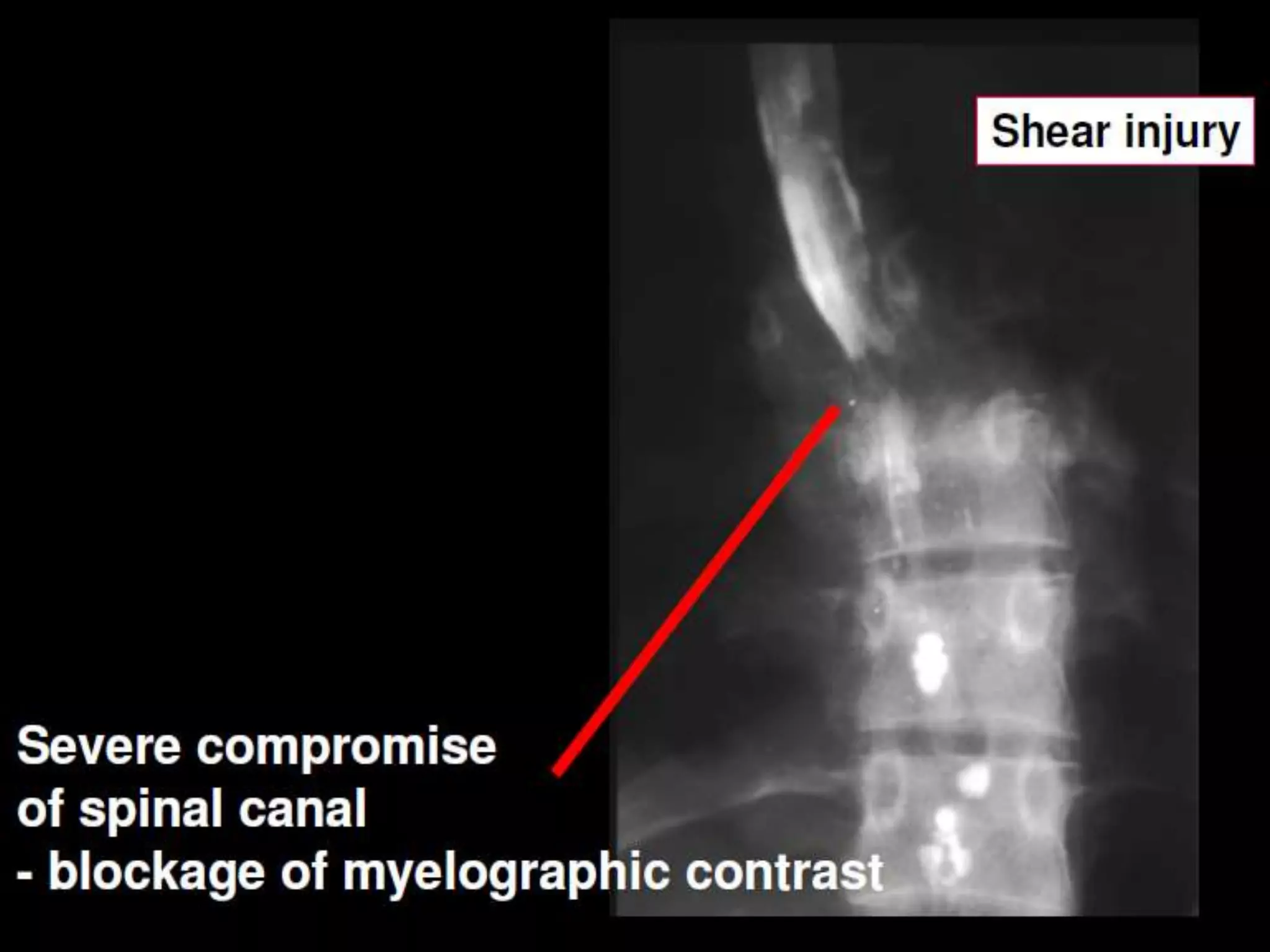
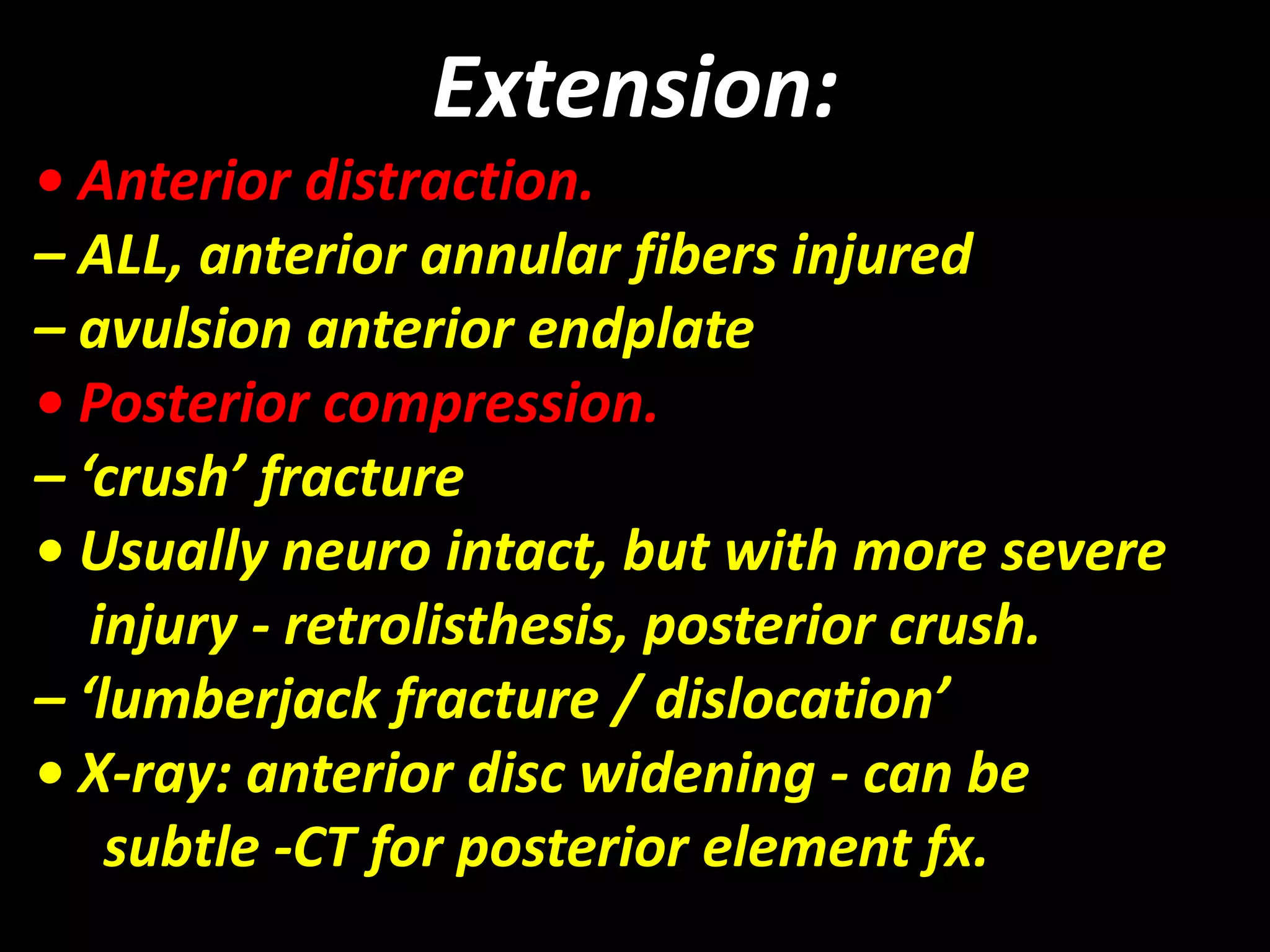
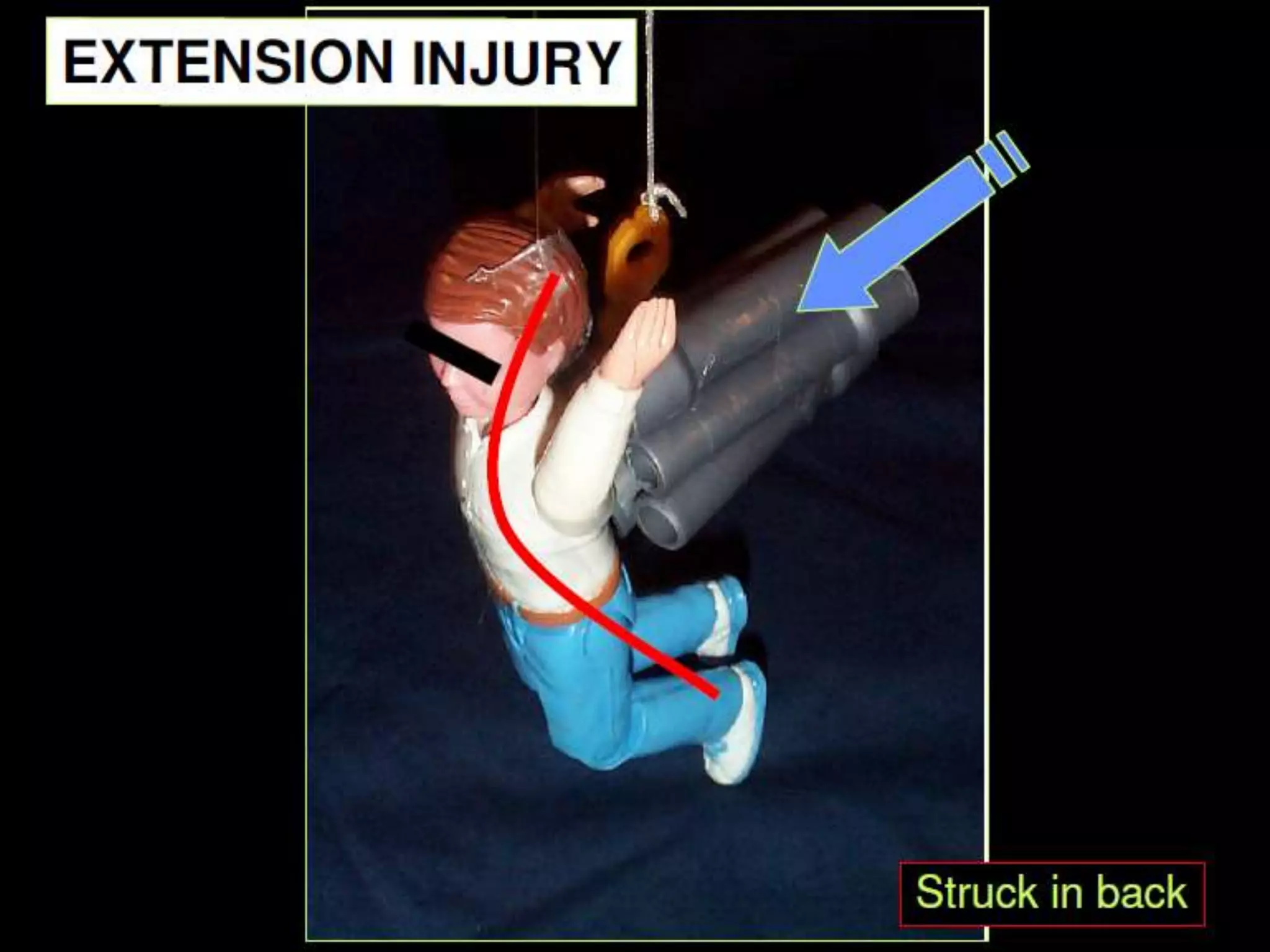
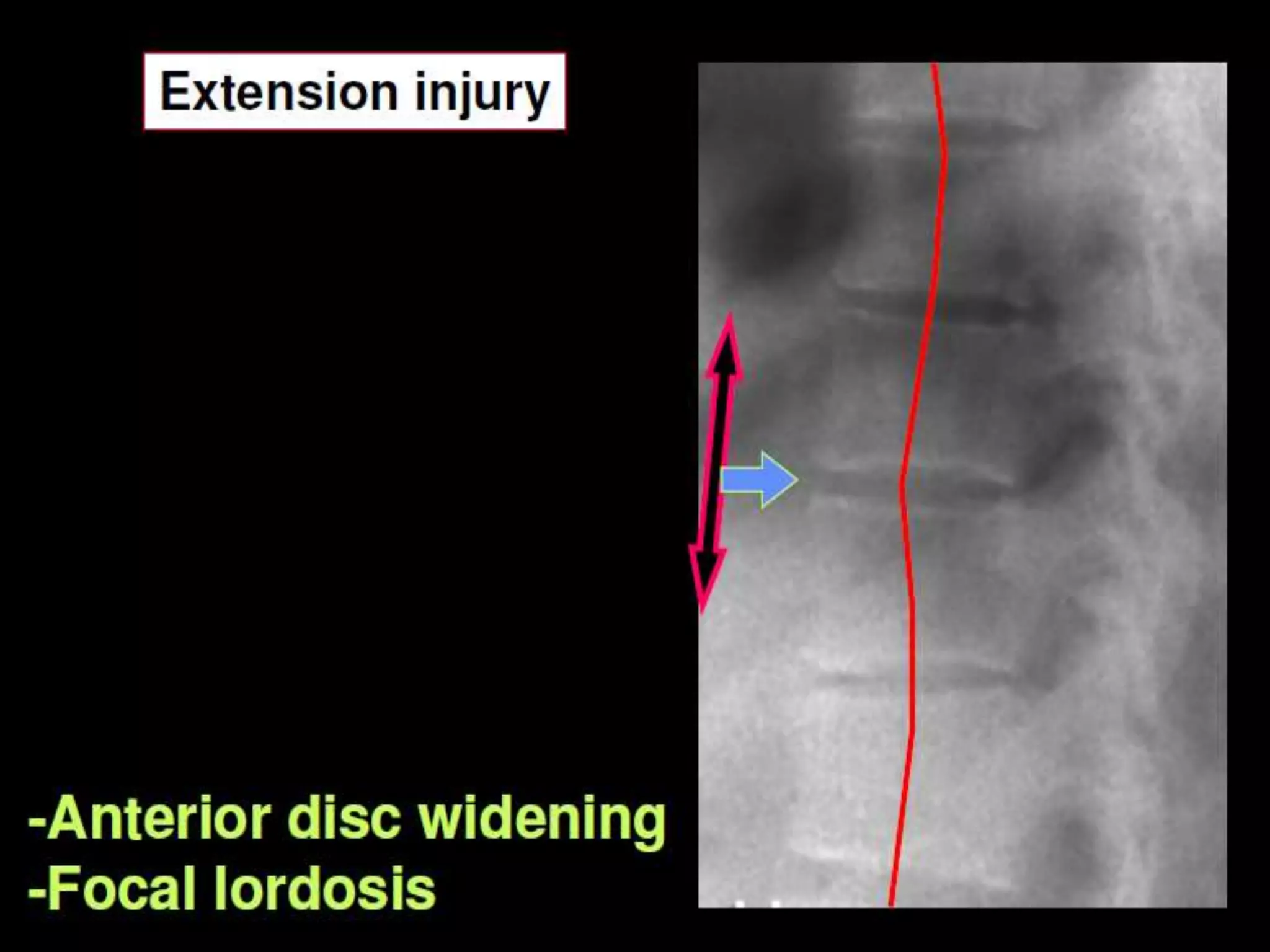
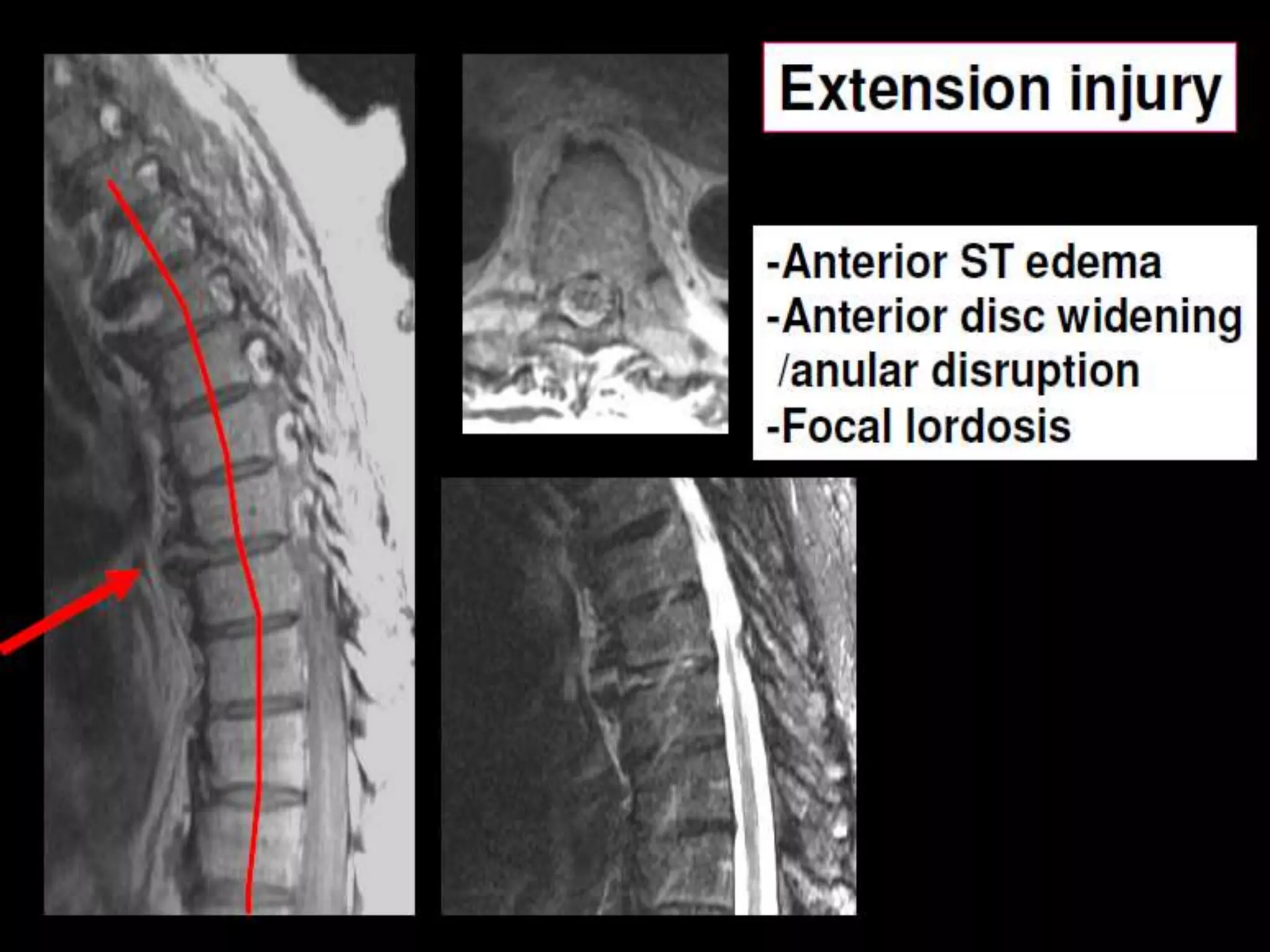
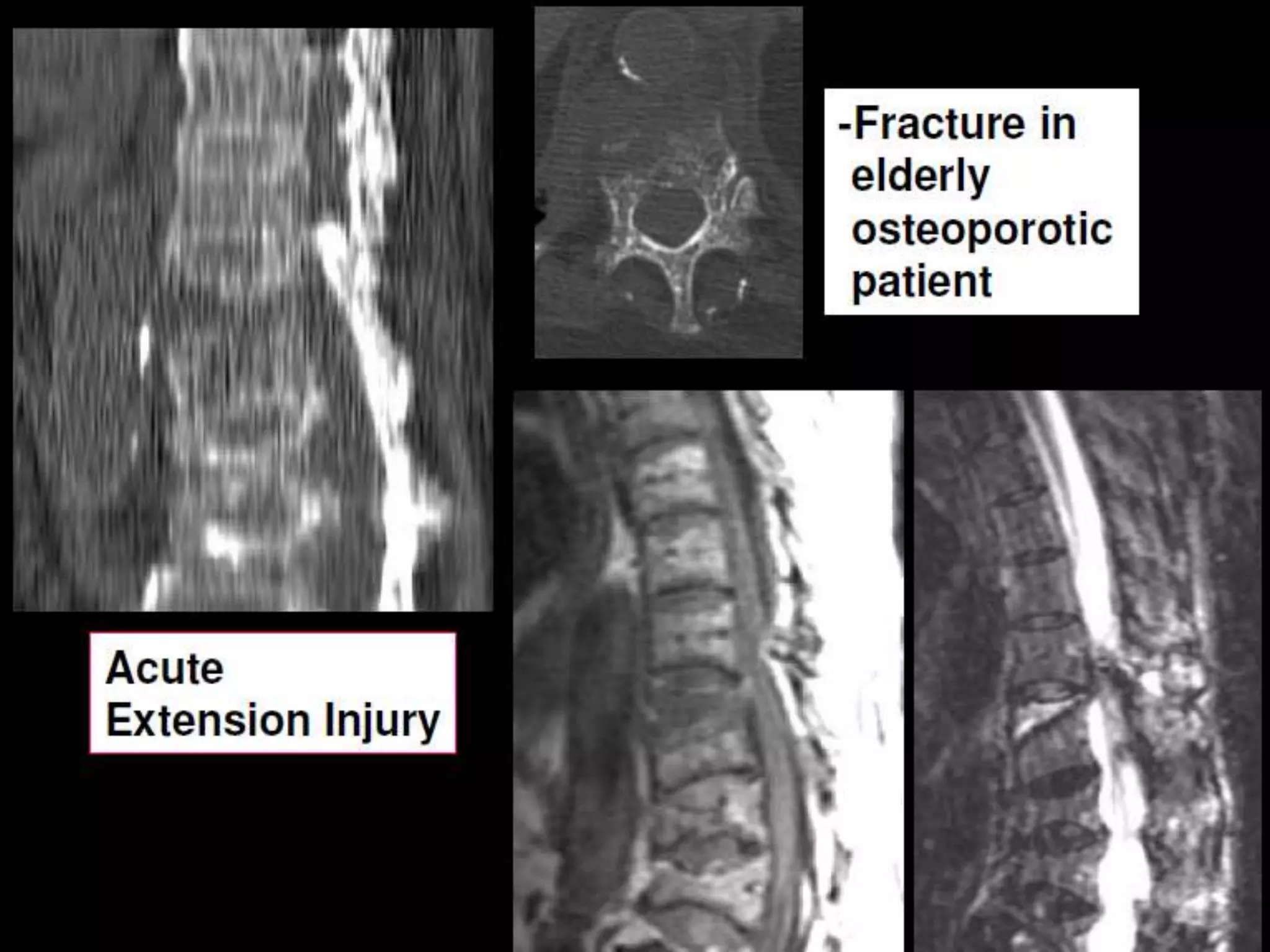
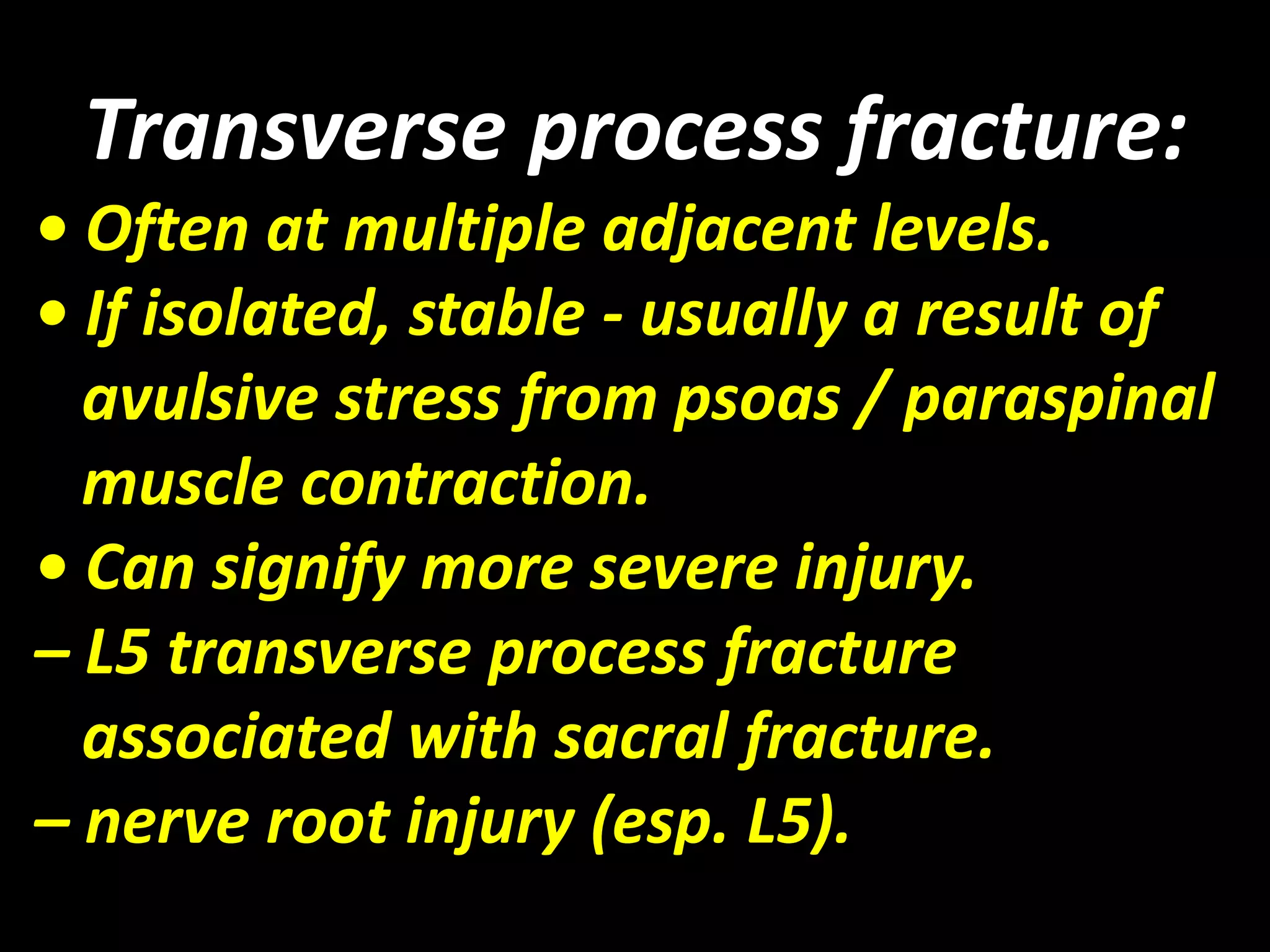
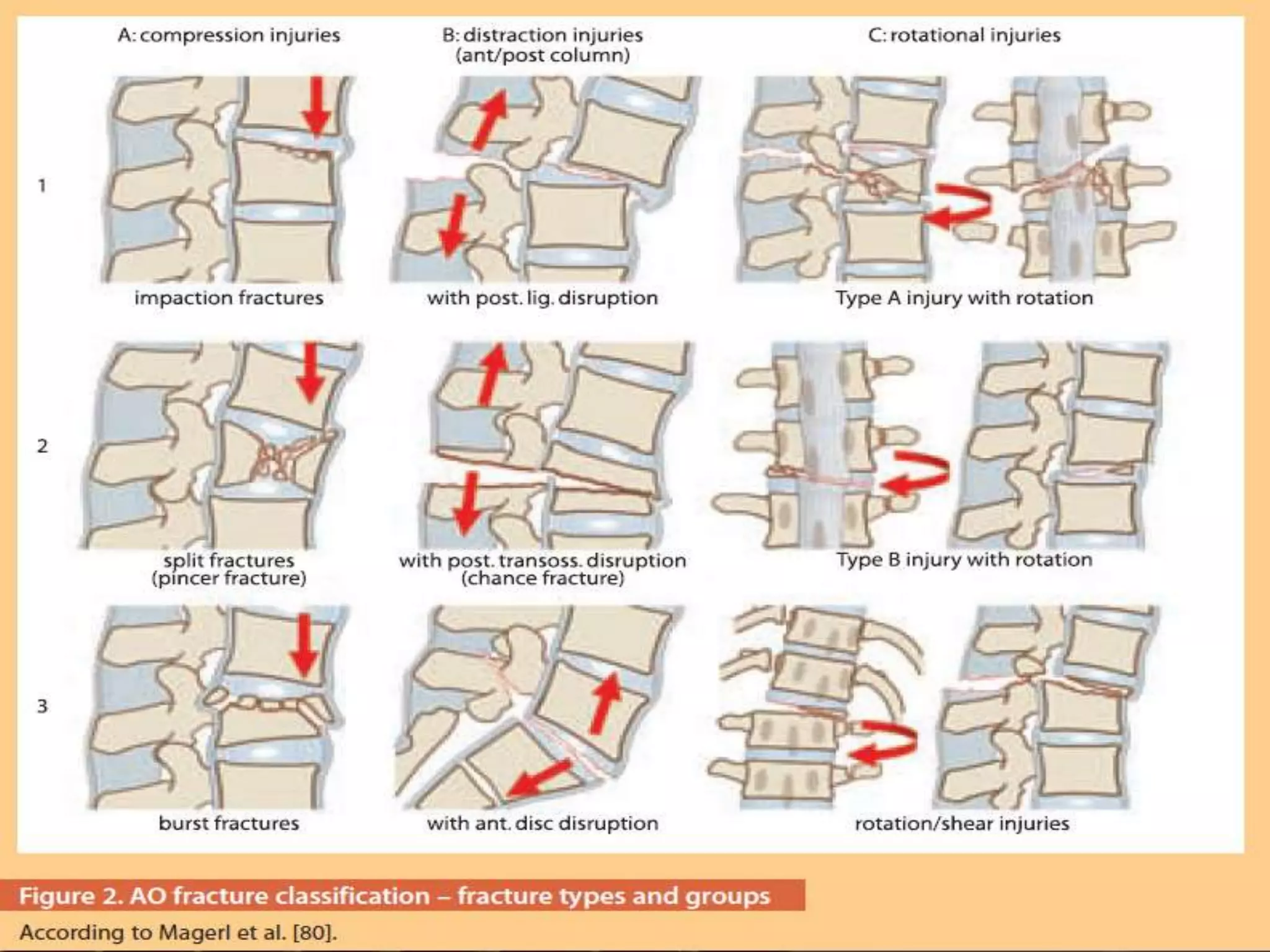
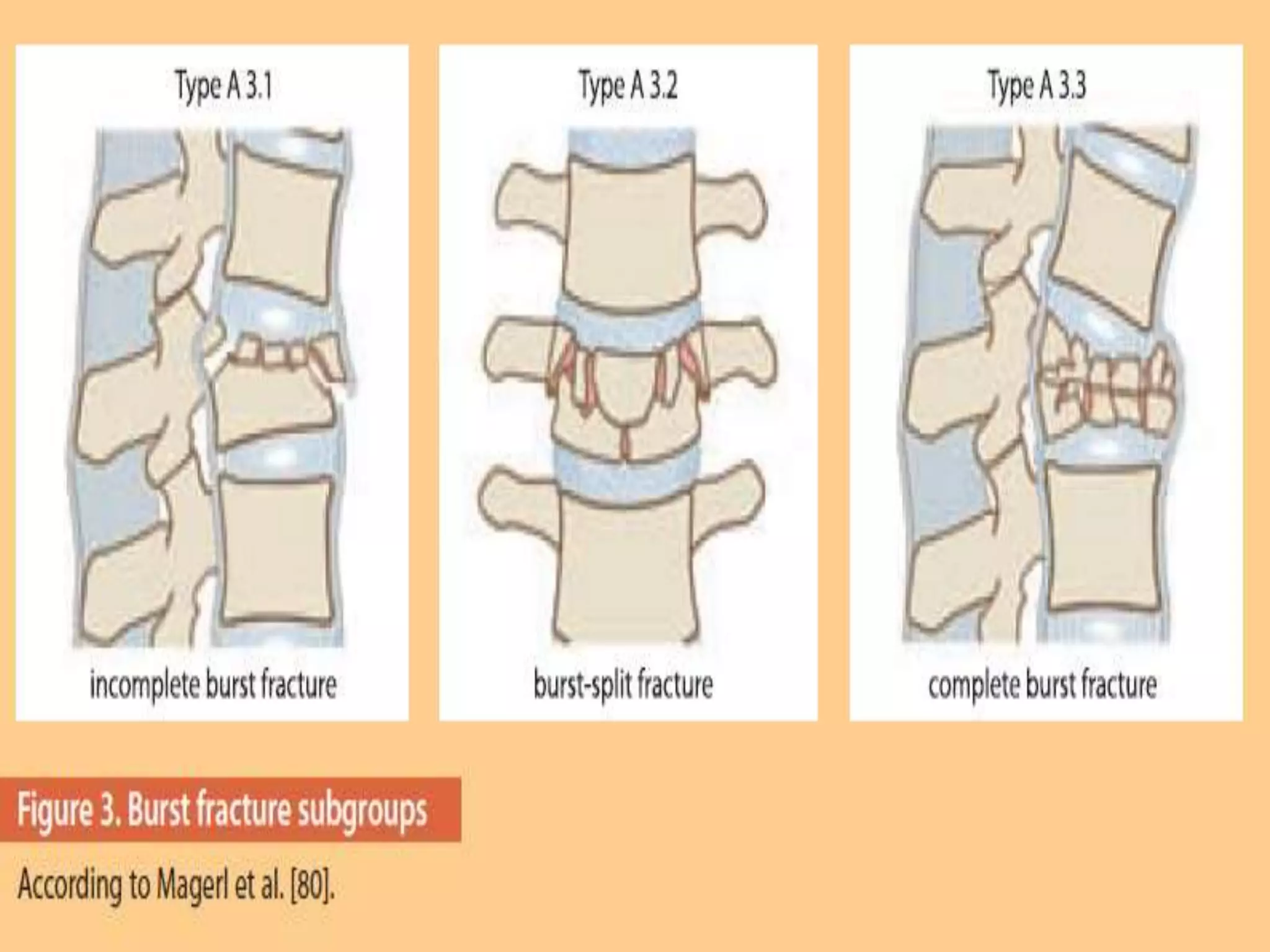
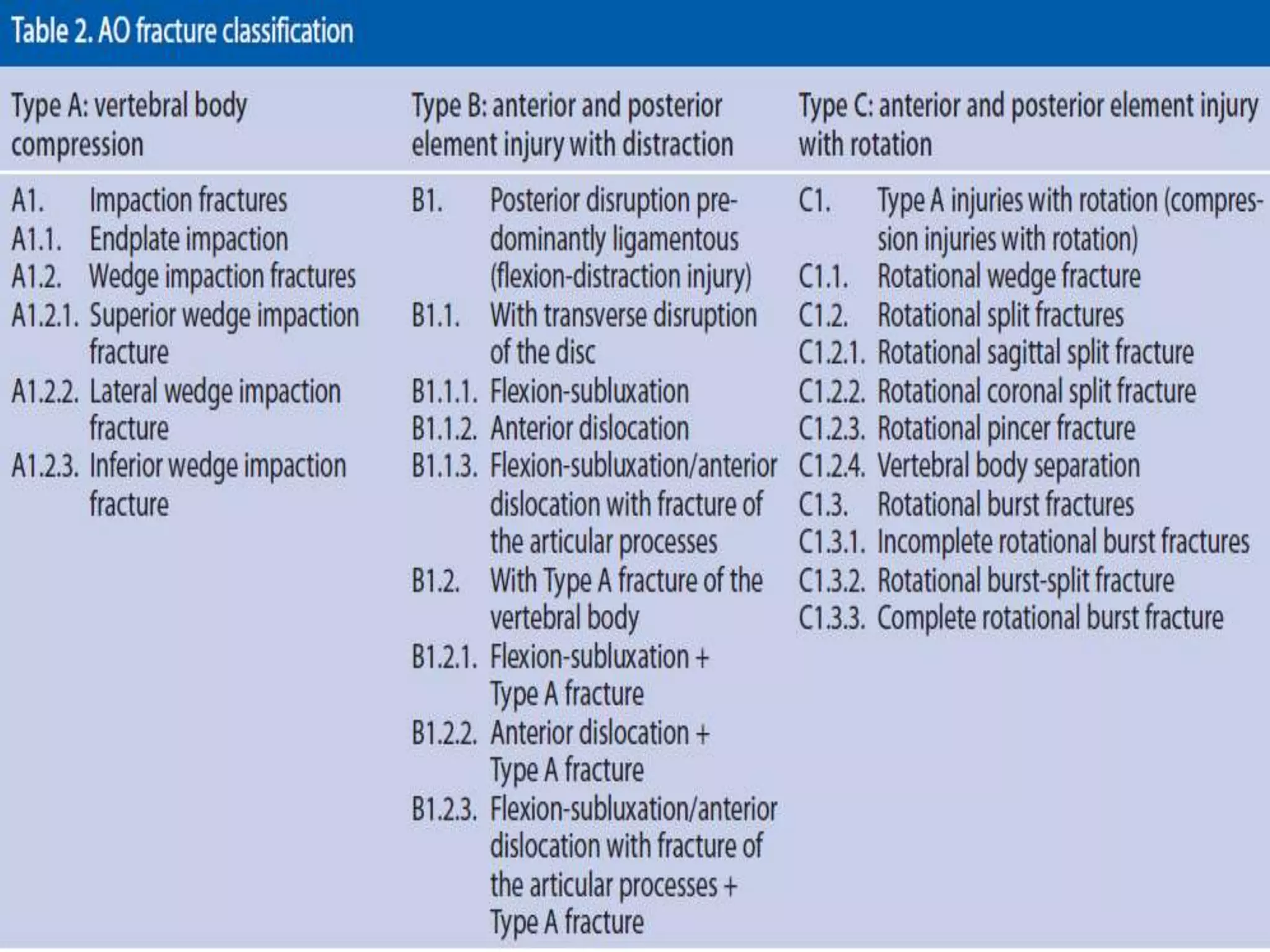
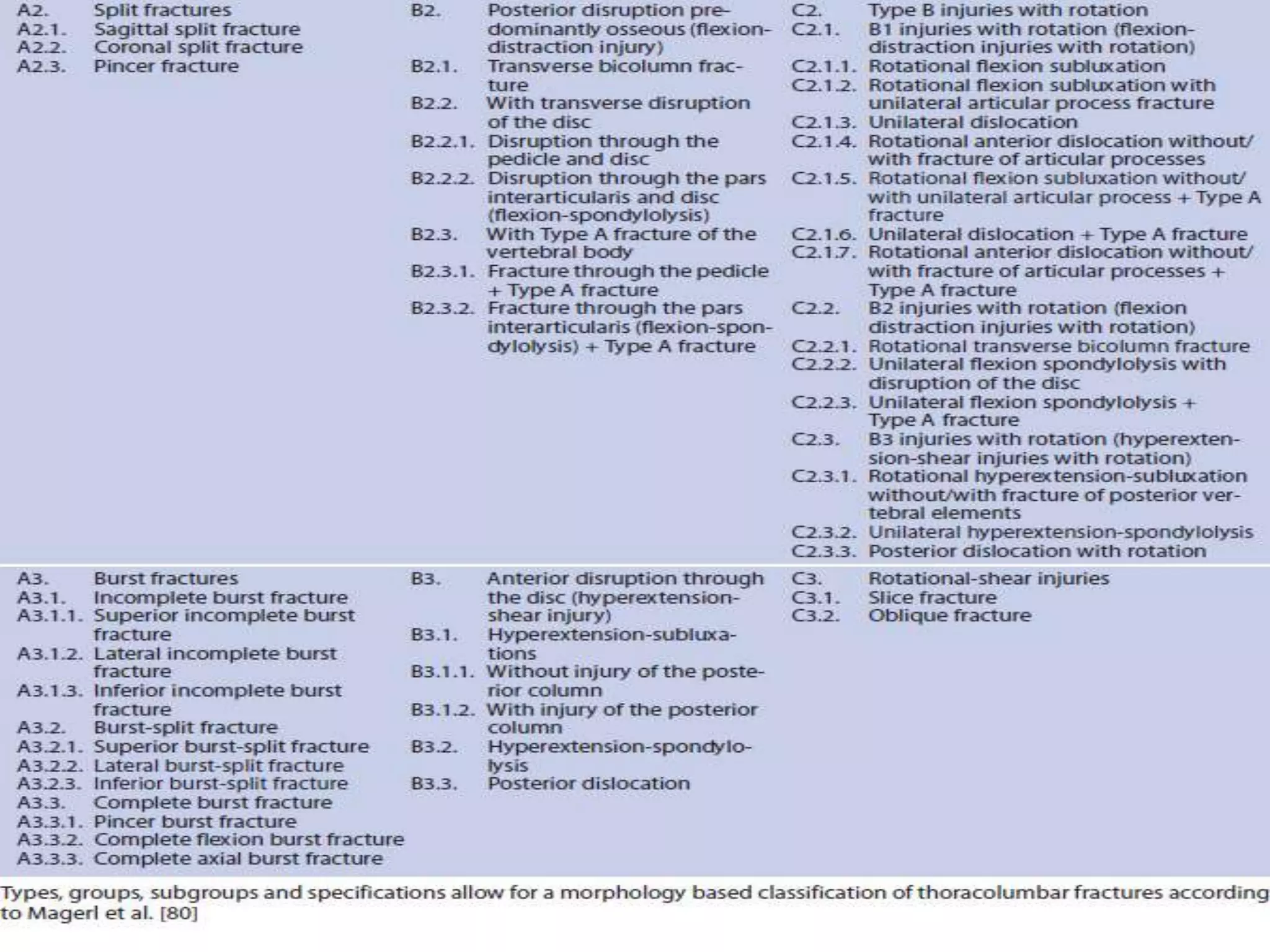

This document discusses radiological imaging of spinal trauma and spinal cord injuries. It describes the common mechanisms of spinal injury including flexion, extension, axial loading, and rotation injuries. It outlines the aims of the radiologist in evaluating spinal trauma to define the extent and type of injury and guide management. The document then focuses on cervical spine trauma, providing details on imaging modalities, injury patterns, classifications of fractures and dislocations, and specific cervical spine injuries associated with different mechanisms. It also discusses thoracolumbar trauma including force vectors, stability considerations, basic fracture patterns, and specific injuries.



































































