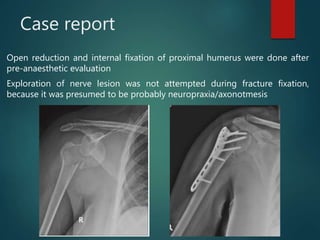
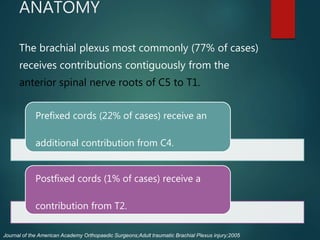
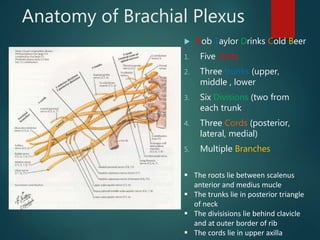
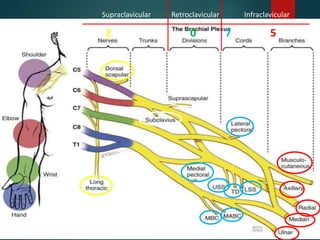
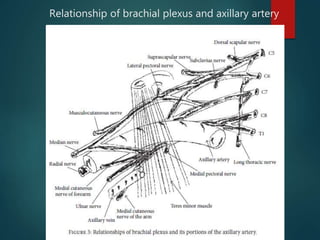
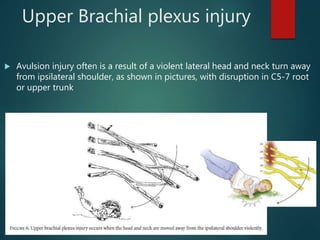
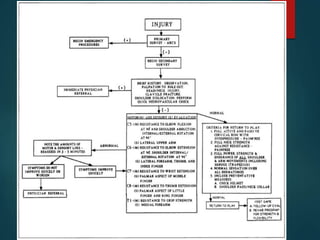
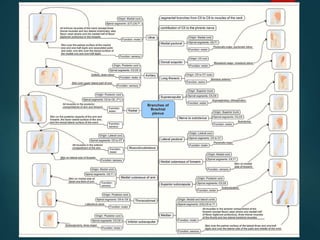
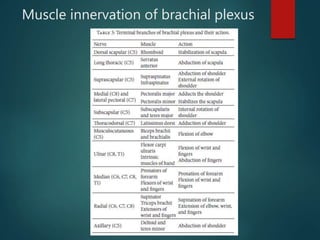
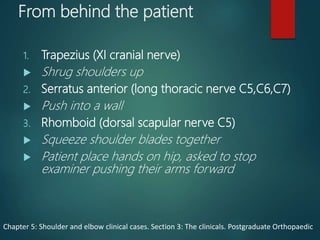
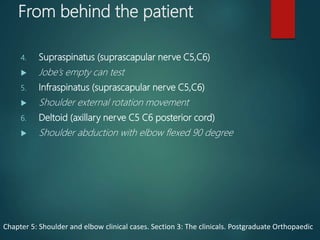
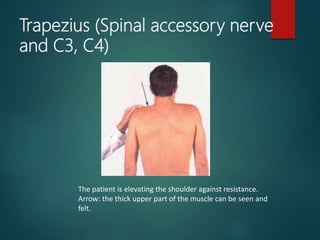
This document presents a case report of a 53-year-old female who sustained a traumatic brachial plexus injury after falling down a flight of stairs. On examination, she had sensory and motor deficits in her right upper limb consistent with an infraclavicular brachial plexus palsy. She underwent conservative therapy including physiotherapy and splinting. Over an 18-month period, her function gradually improved but she was left with some residual weakness. The document discusses the anatomy of the brachial plexus, mechanisms of injury, clinical examination findings, and prognosis factors for peripheral nerve injuries.