The document provides information on spinal cord injury, including:
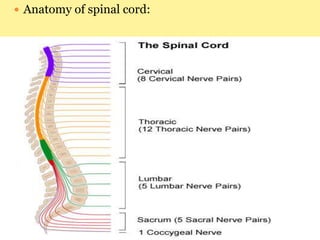
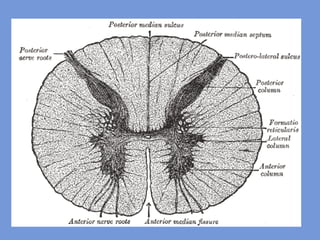
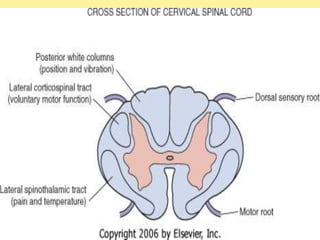
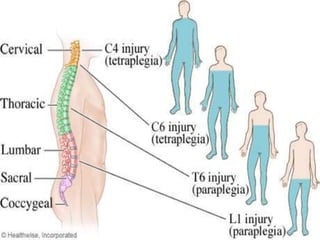
- The anatomy and physiology of the spinal cord, including its segments, grey and white matter, and dermatomes and myotomes.
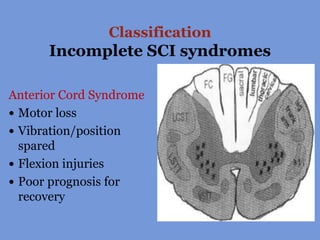
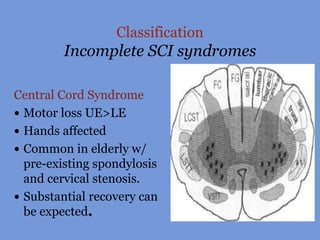
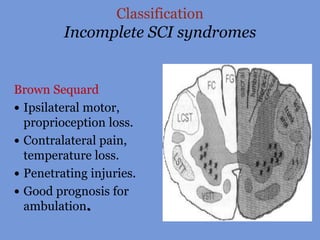
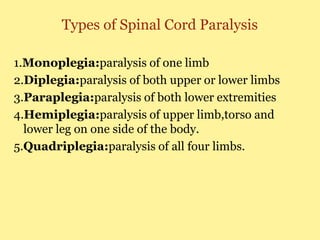
- The classification of spinal cord injuries as complete or incomplete (including types of incomplete injuries like anterior cord syndrome), and types of paralysis.
- The causes, risk factors, signs and symptoms, diagnostic tests, and medical and surgical management of spinal cord injuries.
- Nursing diagnoses and complications related to spinal cord injuries.




![Spinal cord injury [recovered]](https://cdn.slidesharecdn.com/ss_thumbnails/spinalcordinjuryrecovered-201022180848-thumbnail.jpg?width=640&height=640&fit=bounds)


































































![Cells and Organs of immune system [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/cellsandorgansofimmunesystemautosaved-260123152717-ea0cb261-thumbnail.jpg?width=640&height=640&fit=bounds)
















