
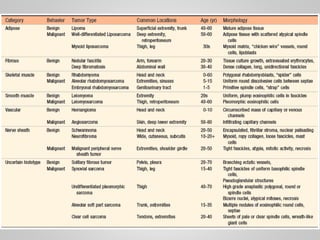



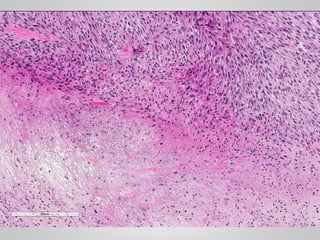



- Soft tissue tumors arise from non-epithelial connective tissues like fat, muscle, fibrous tissues, blood vessels, or deep skin tissues. They represent less than 1% of cancers. - Soft tissue tumors are classified based on the tissue of origin and characteristics like morphology, immunohistochemistry, and genetics. Major categories include adipose, fibrous, skeletal muscle, smooth muscle, and tumors of uncertain origin. - Specific tumor types discussed in detail include lipoma, liposarcoma, nodular fasciitis, fibromatosis, rhabdomyosarcoma, leiomyoma, leiomyosarcoma, synovial sarcoma, and undifferent























































































