






















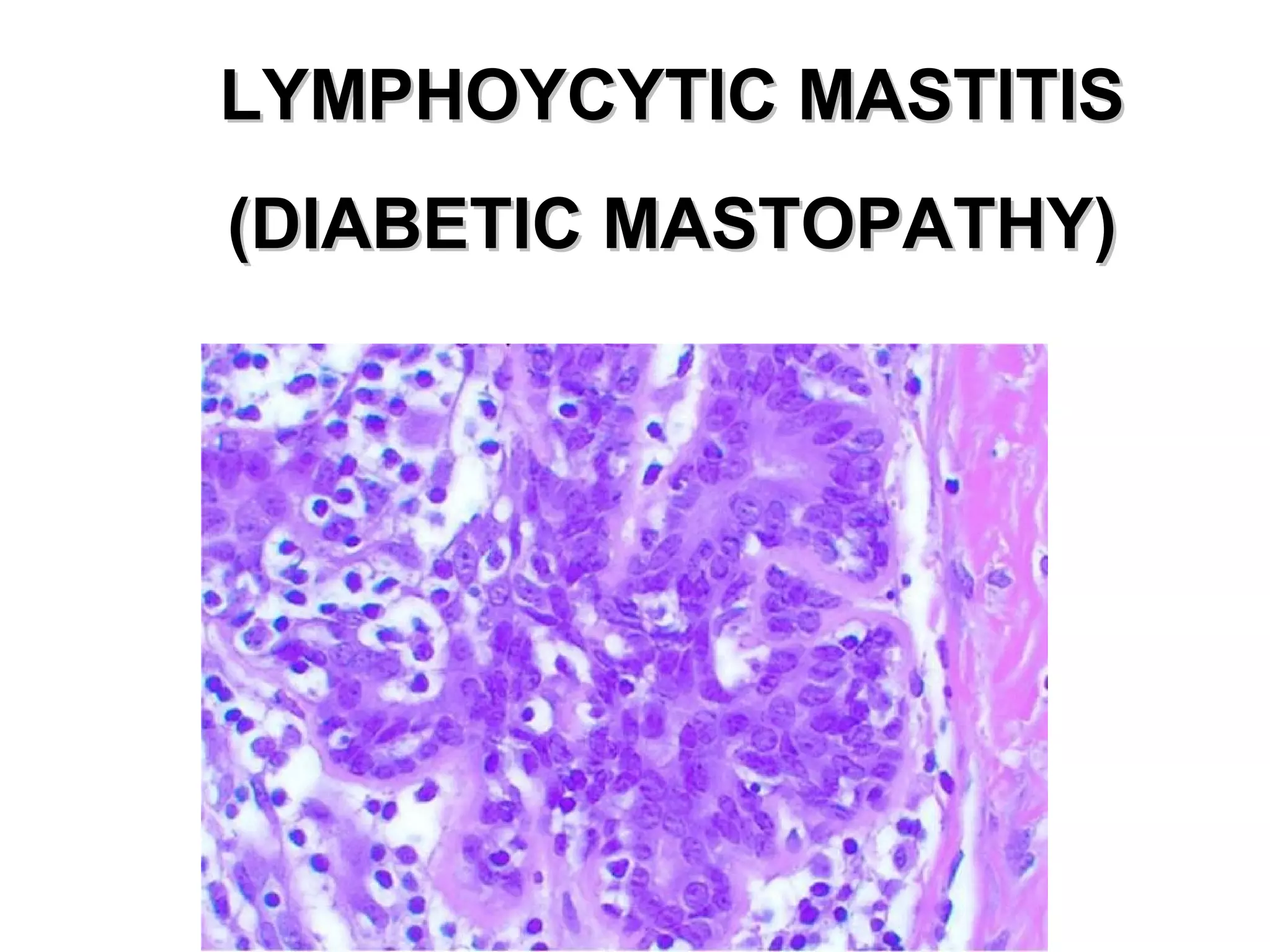





















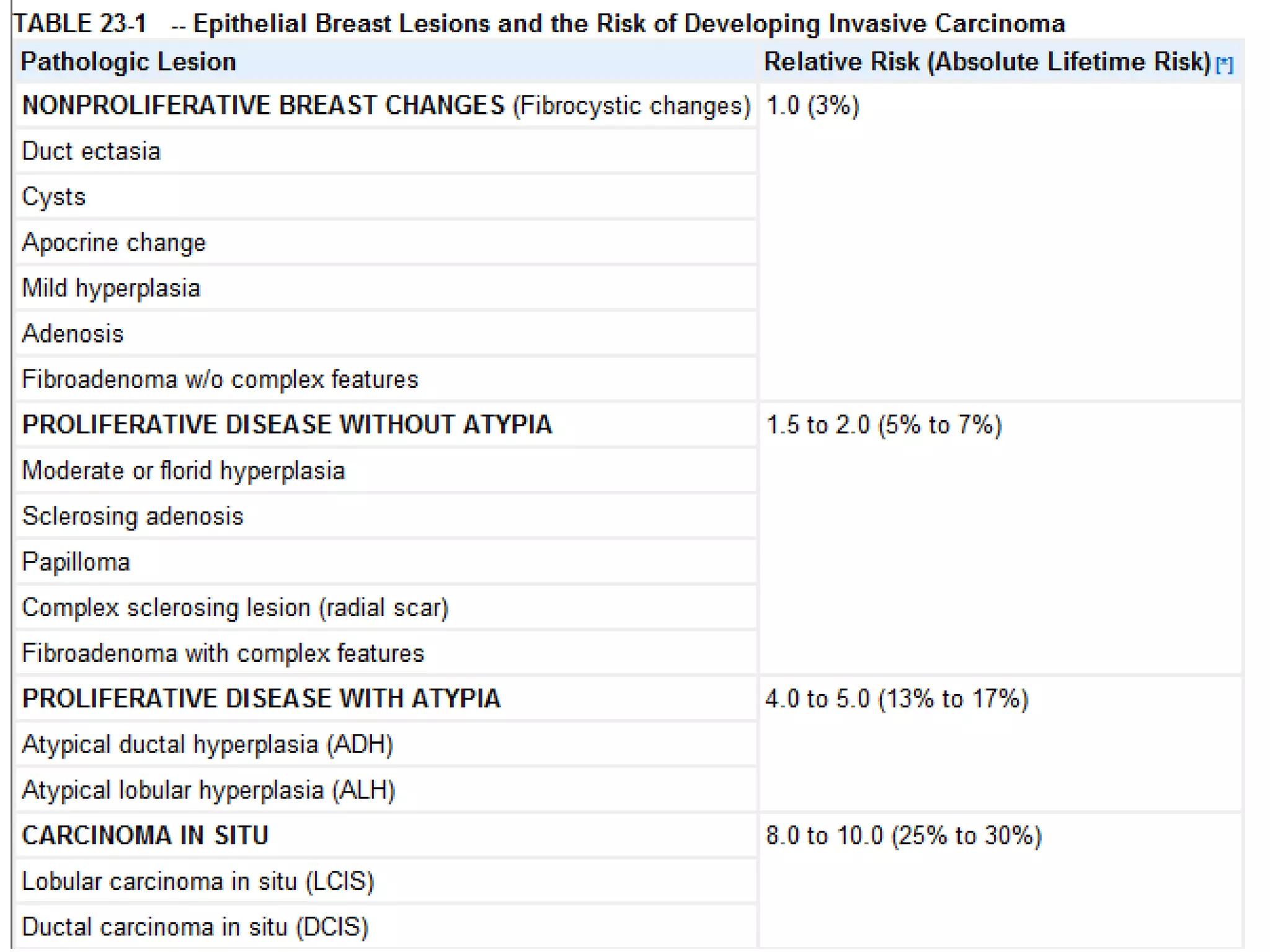

This document discusses non-neoplastic lesions of the breast. It begins by describing the histology of the breast including lobes, lobules, acini/alveoli, and ducts. It then covers developmental variations such as milkline remnants, accessory breast tissue, nipple inversion, and macromastia. Various types of inflammation are also discussed such as acute mastitis, periductal inflammation, duct ectasia, fat necrosis, and granulomatous mastitis. Other non-neoplastic lesions covered include cysts, adenosis, fibrosis, ductal hyperplasia, papillomas, and atypical hyperplasia. Key histological features of atypia are highlighted.























































































