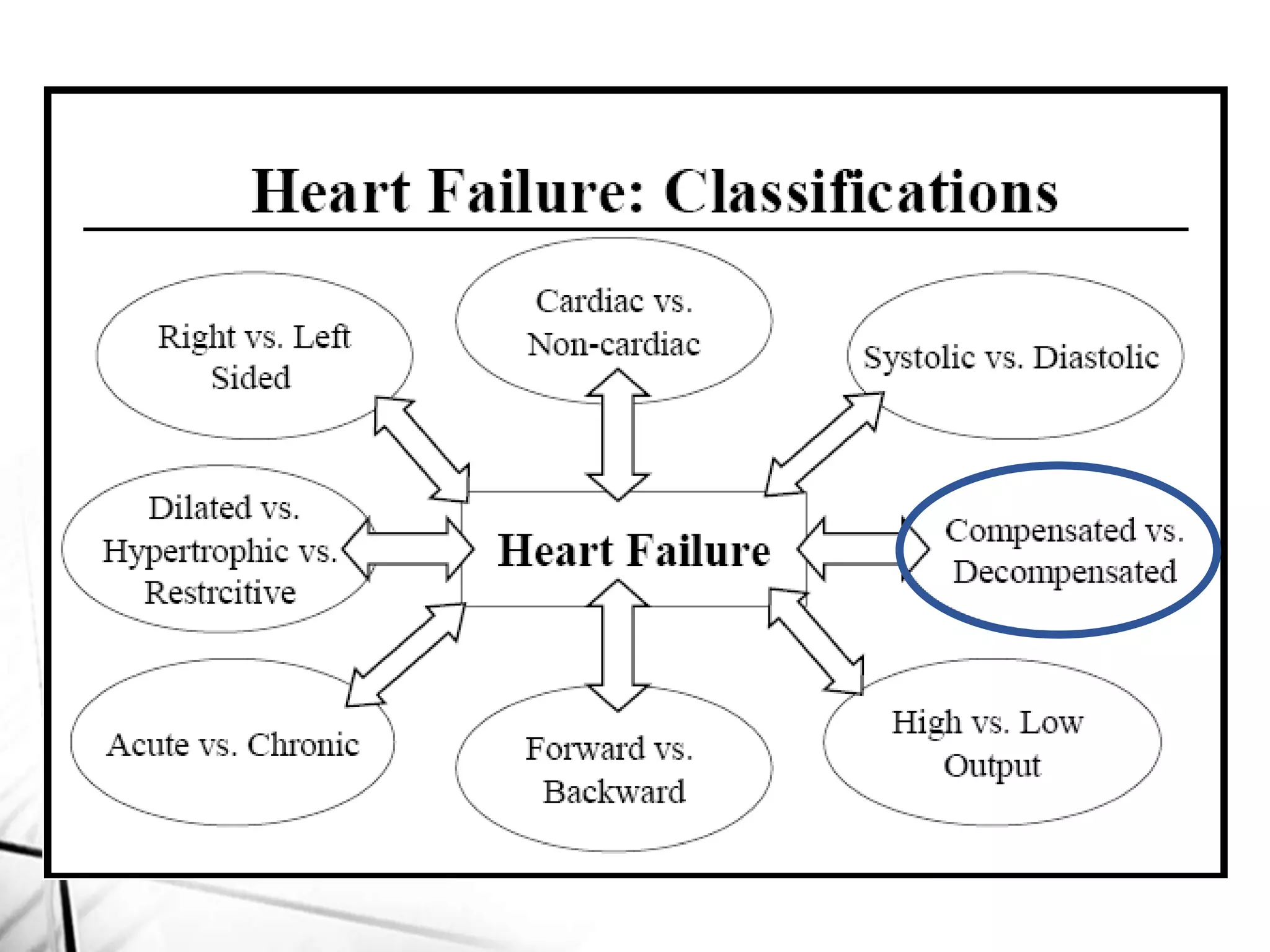
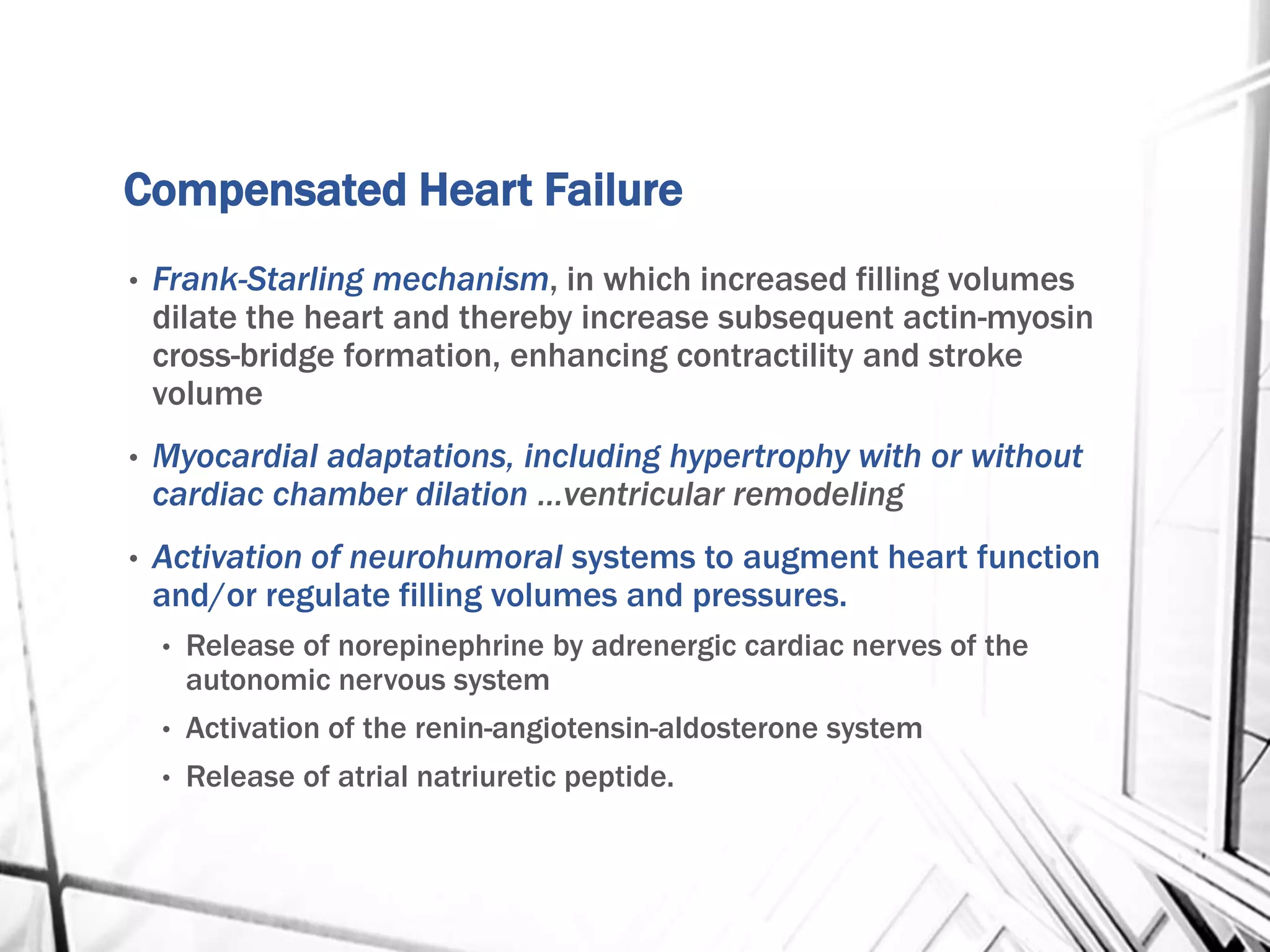
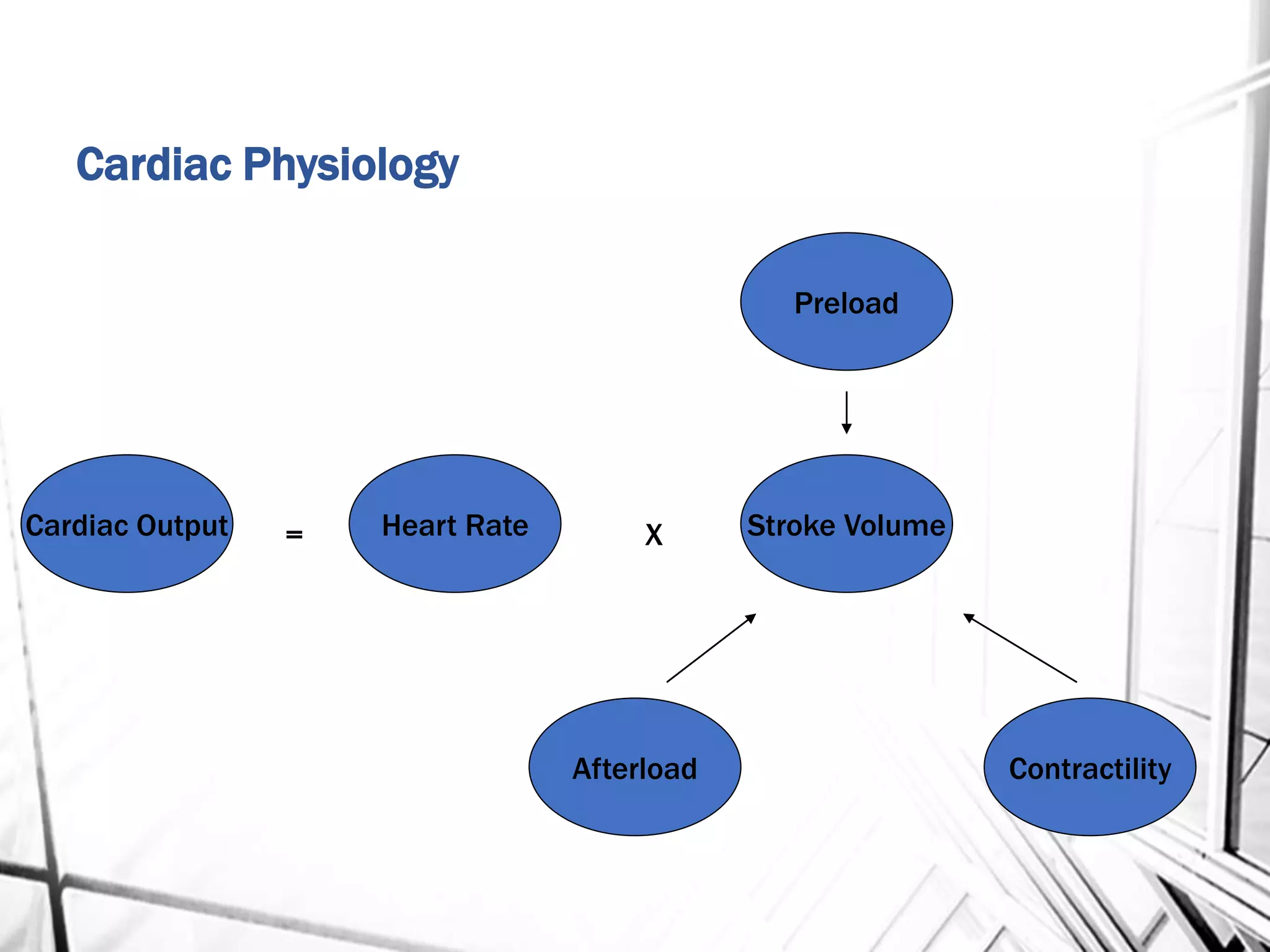



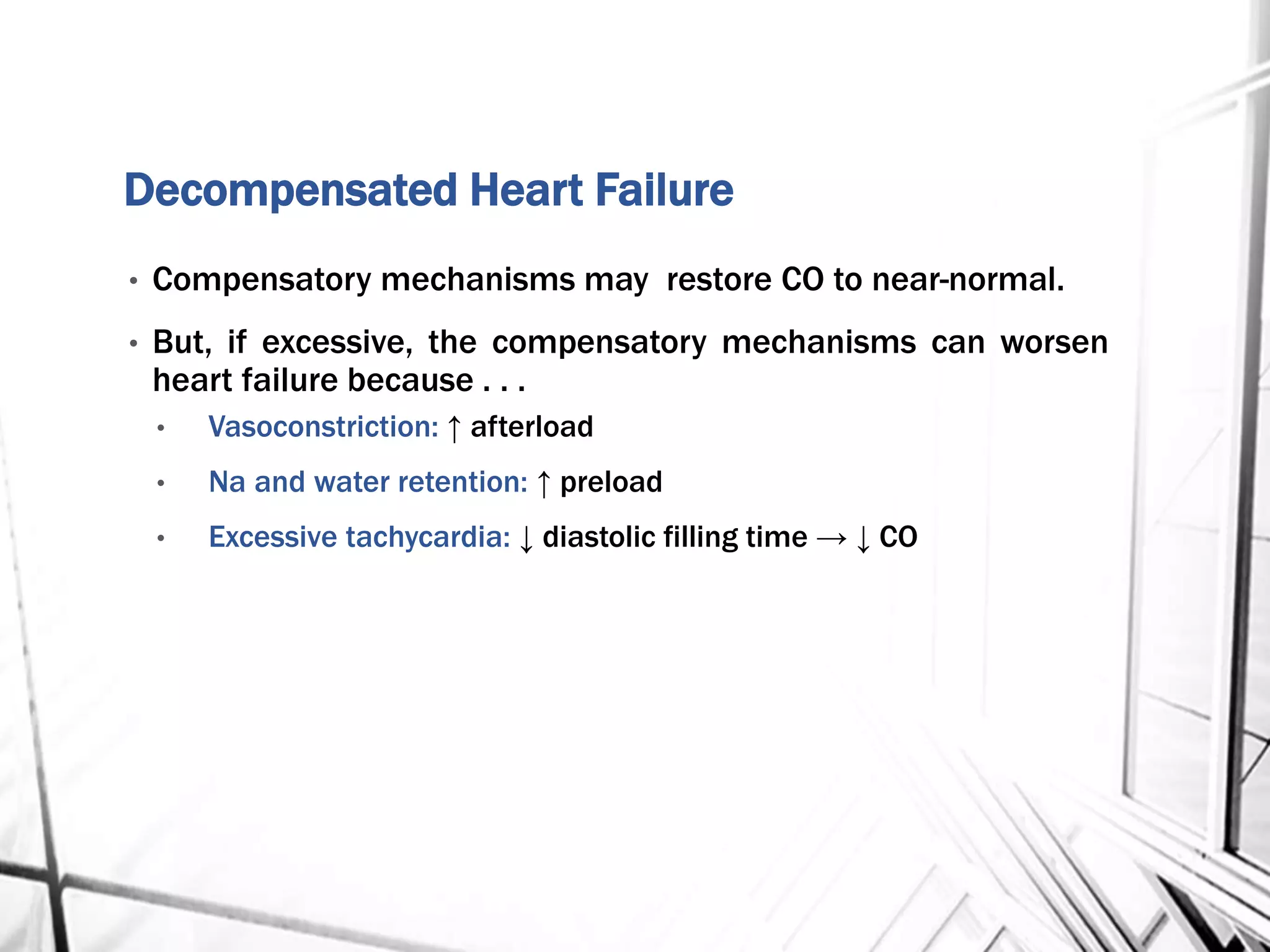
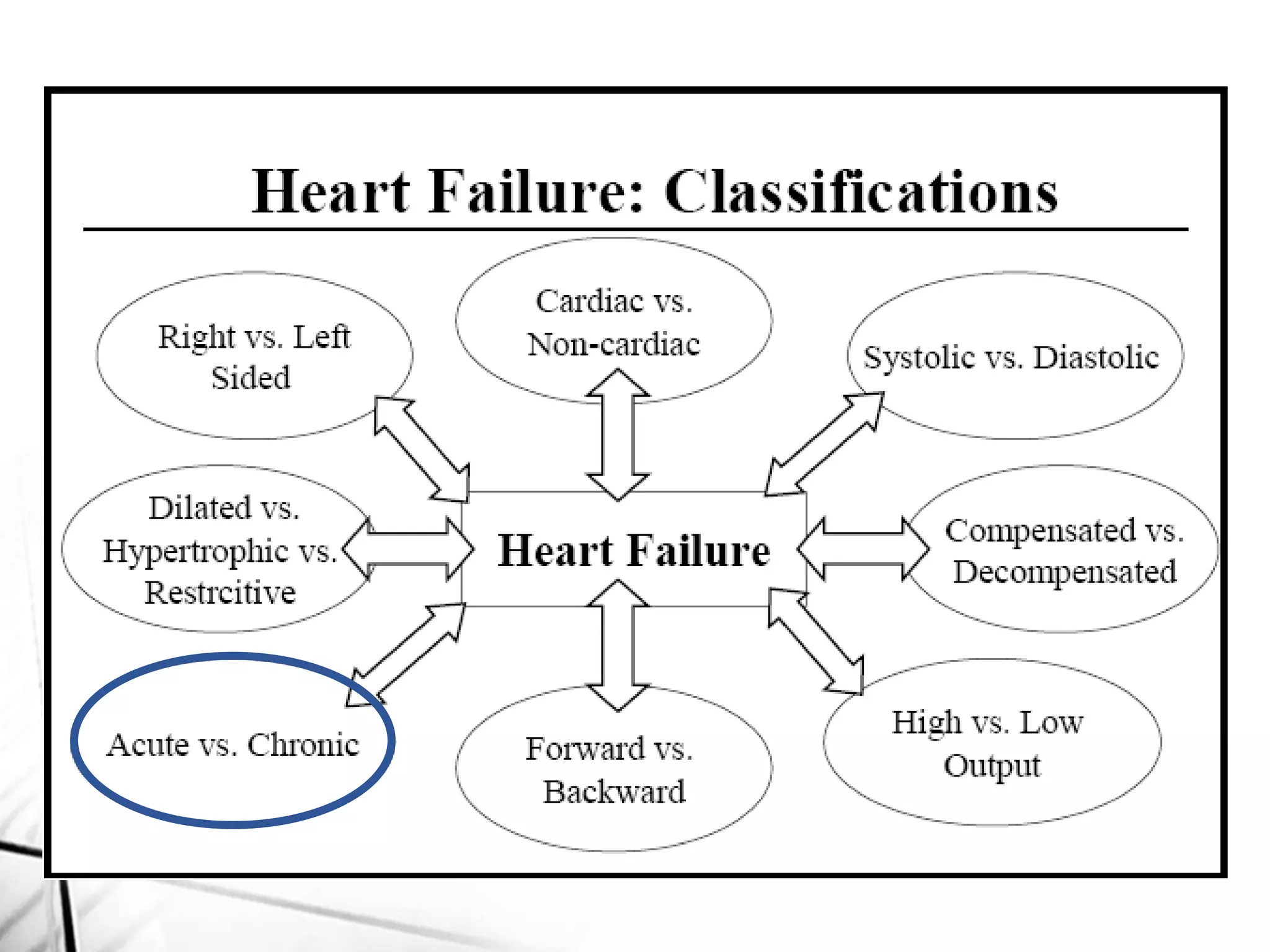














This document provides information on heart failure (CHF), including: 1) CHF is a clinical syndrome that results from any structural or functional cardiac disorder that impairs the ventricle's ability to fill or eject blood. 2) The main mechanisms of CHF are increased blood volume, increased resistance to blood flow, decreased contractility, and decreased filling. 3) CHF can be compensated initially through mechanisms like the Frank-Starling mechanism and neurohormonal activation, but these can eventually worsen heart failure.