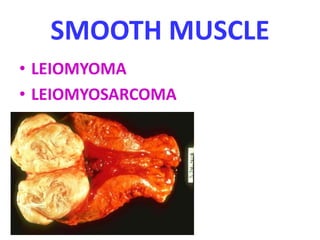
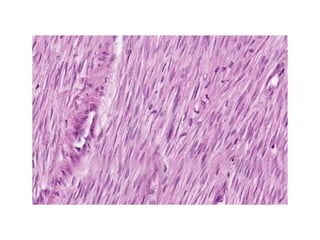
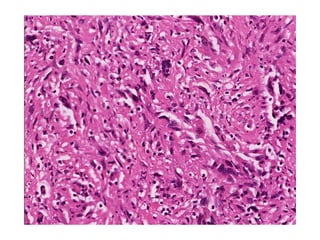
1. Soft tissue tumors can arise from adipose, fibrous, skeletal muscle, smooth muscle, vascular, and peripheral nerve tissues. They range from benign to malignant.
2. Malignant soft tissue tumors are graded I-III based on differentiation, with grades I-II having potential for recurrence but low risk of metastasis. Prognosis depends on histologic type, grade, size, and anatomic site.
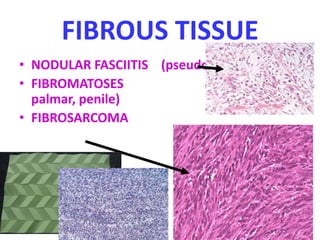
3. Examples of benign and malignant soft tissue tumors mentioned include lipomas and liposarcomas of adipose tissue, nodular fasciitis and fibrosarcomas of fibrous tissue, and rhabdomyomas and rhabdomyosarcomas of skeletal