
Downloaded 318 times





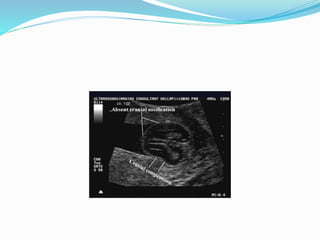




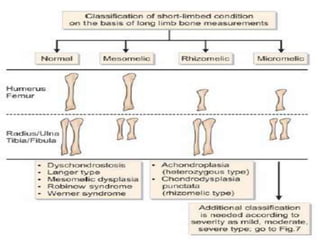
This document summarizes several skeletal dysplasias that can be observed on prenatal ultrasound. It describes key features and prognosis for conditions including achondrogenesis, thanatophoric dysplasia, campomelic dysplasia, osteogenesis imperfecta, hypophosphatasia, asphyxiating thoracic dystrophy, diastrophic dysplasia, chondrodysplasia punctata, kniest dysplasia, isolated limb reduction, robert's syndrome, femur-fibula-ulna syndrome, holt-oram syndrome, thrombocytopenia absent radius syndrome, and cleidocranial dystosis. Many of these conditions are lethal, while others may






















































































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)











