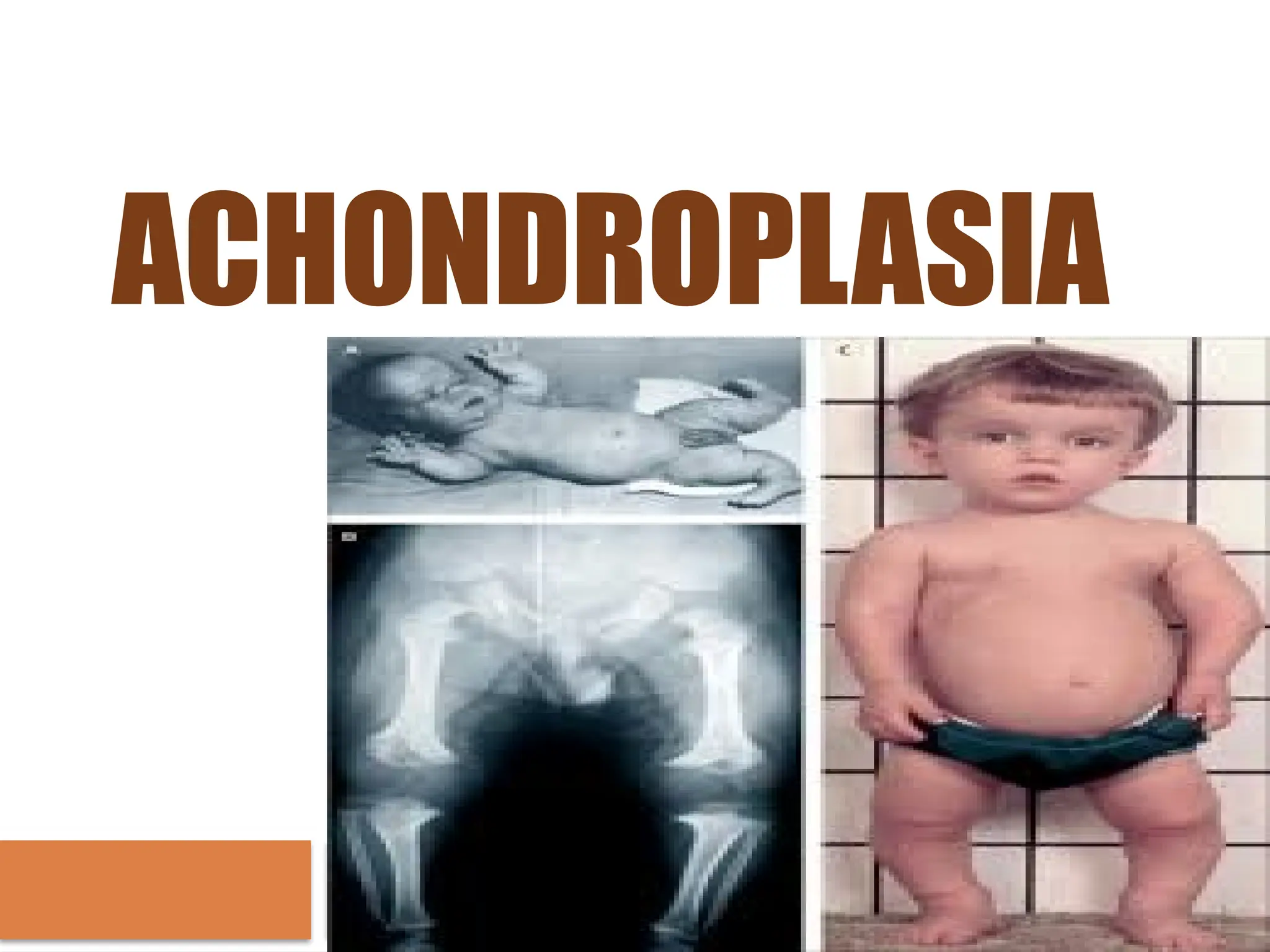
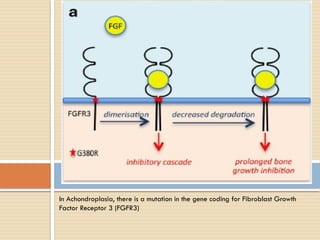
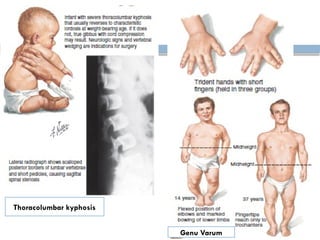
Achondroplasia is the most common skeletal dysplasia characterized by short stature and distinctive craniofacial skeletal features due to a mutation in the FGFR3 gene. It is typically inherited in an autosomal dominant manner, with 90% of cases arising from spontaneous mutations, affecting approximately 10,000 individuals in the U.S. Diagnosis involves history taking, physical examination, laboratory tests, and radiographic findings, with management strategies focused on addressing clinical manifestations, including growth hormone therapy and monitoring for potential complications.















































































![CASE_PRESENTATION_ON_subdural_hematoma(SDH)[1 FINAL PPT]-1.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/casepresentationonsubduralhematomasdh1finalppt-1-260129172522-d405d375-thumbnail.jpg?width=640&height=640&fit=bounds)












