Downloaded 20 times
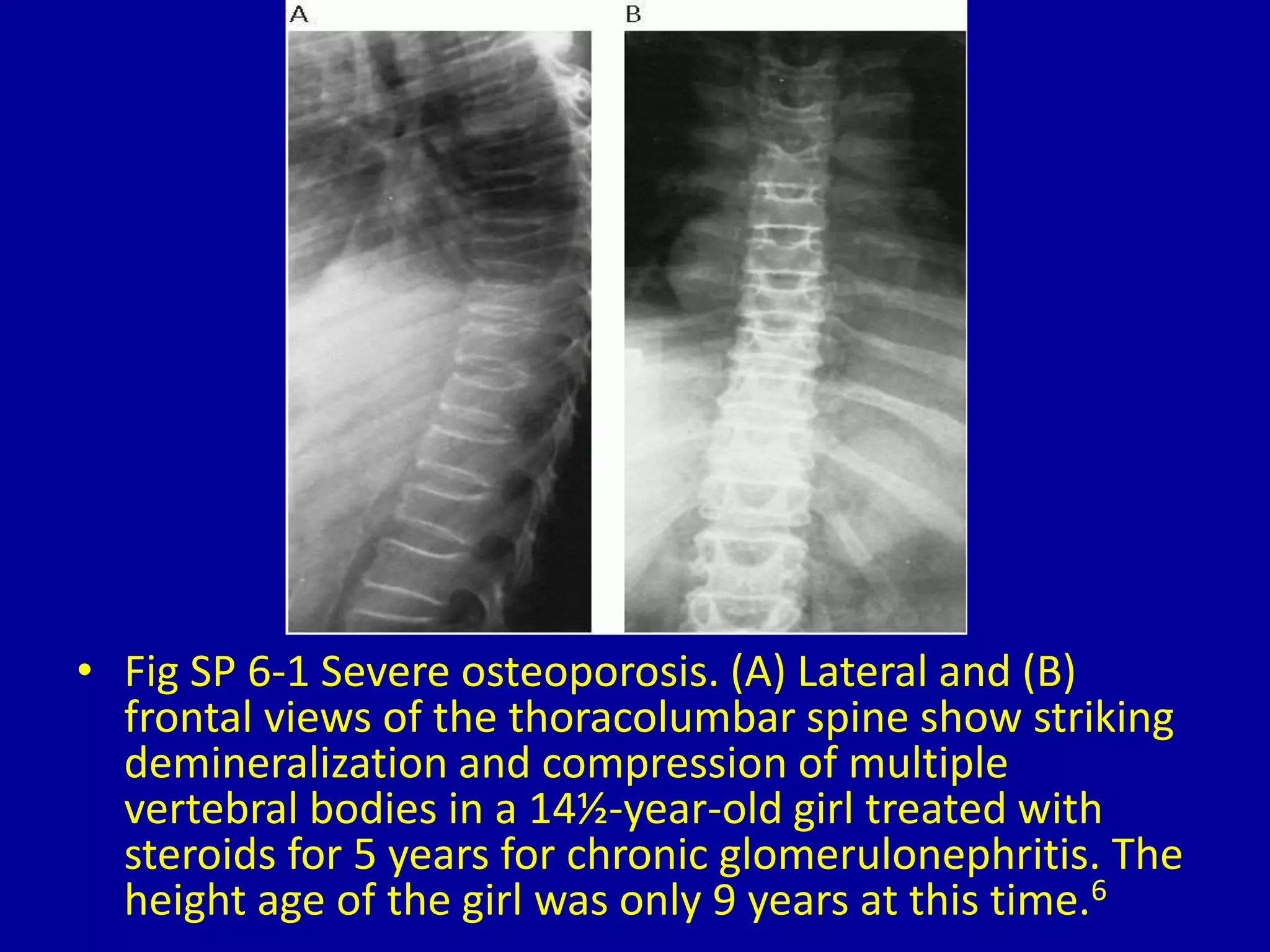
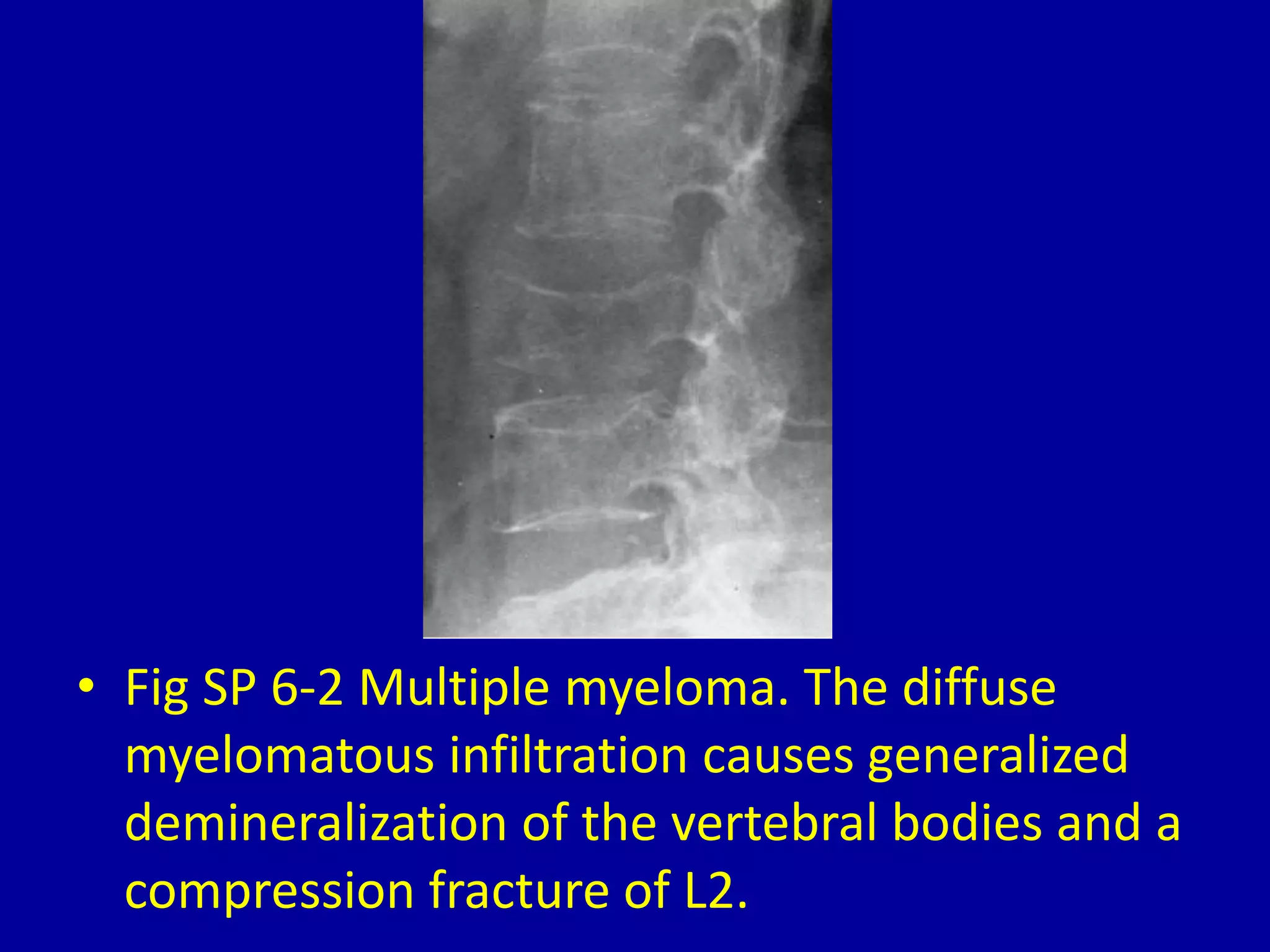
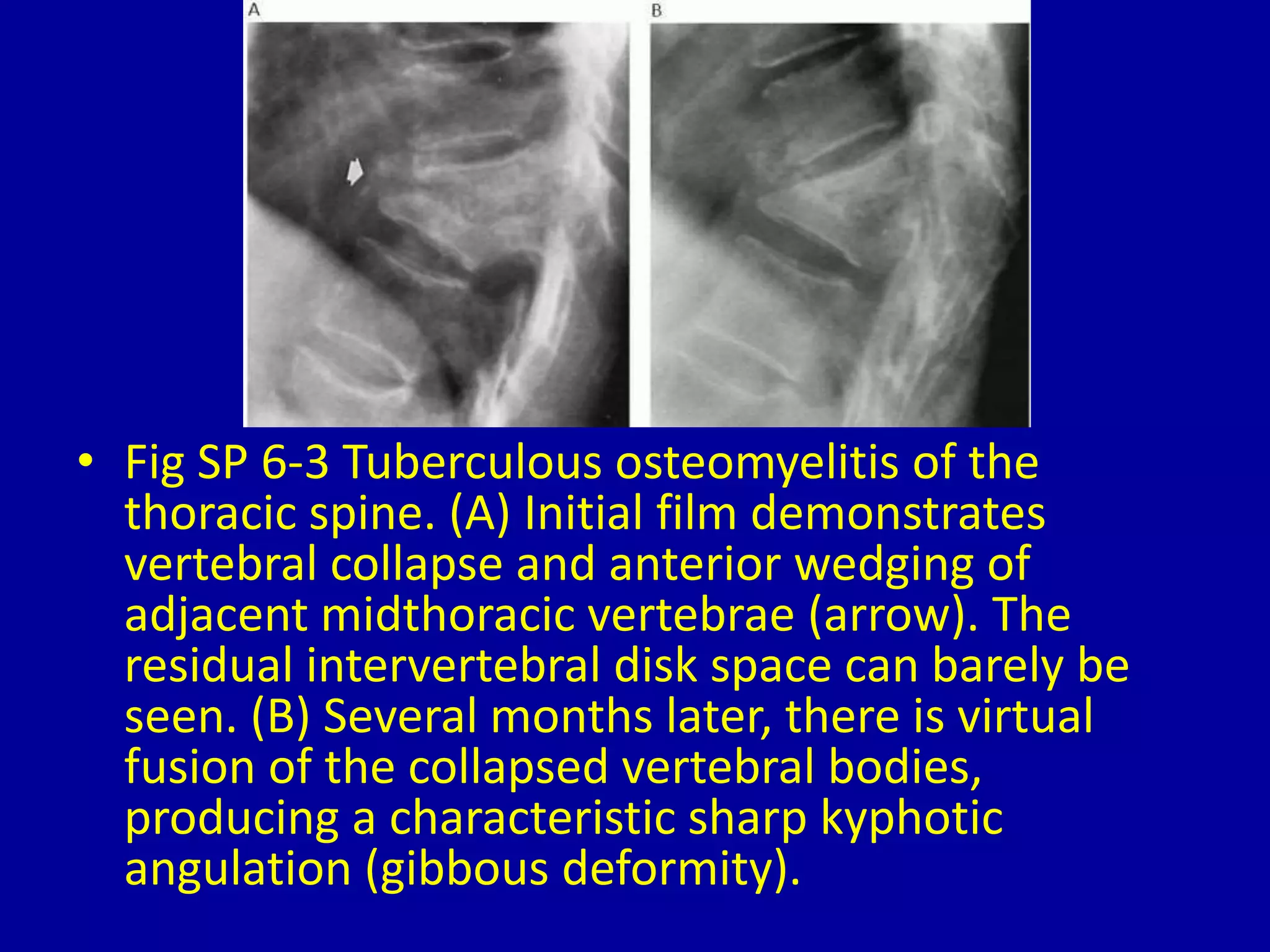

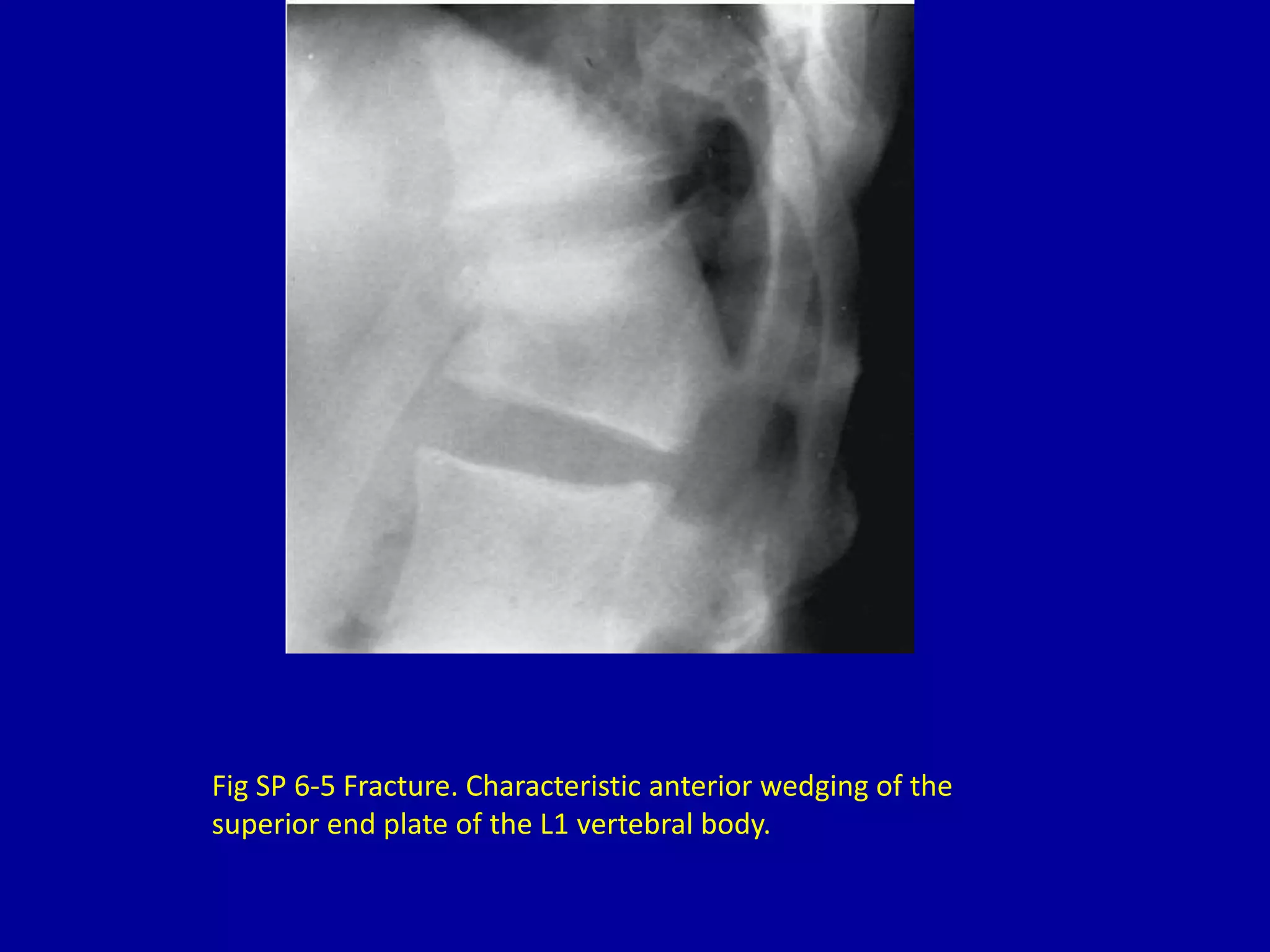
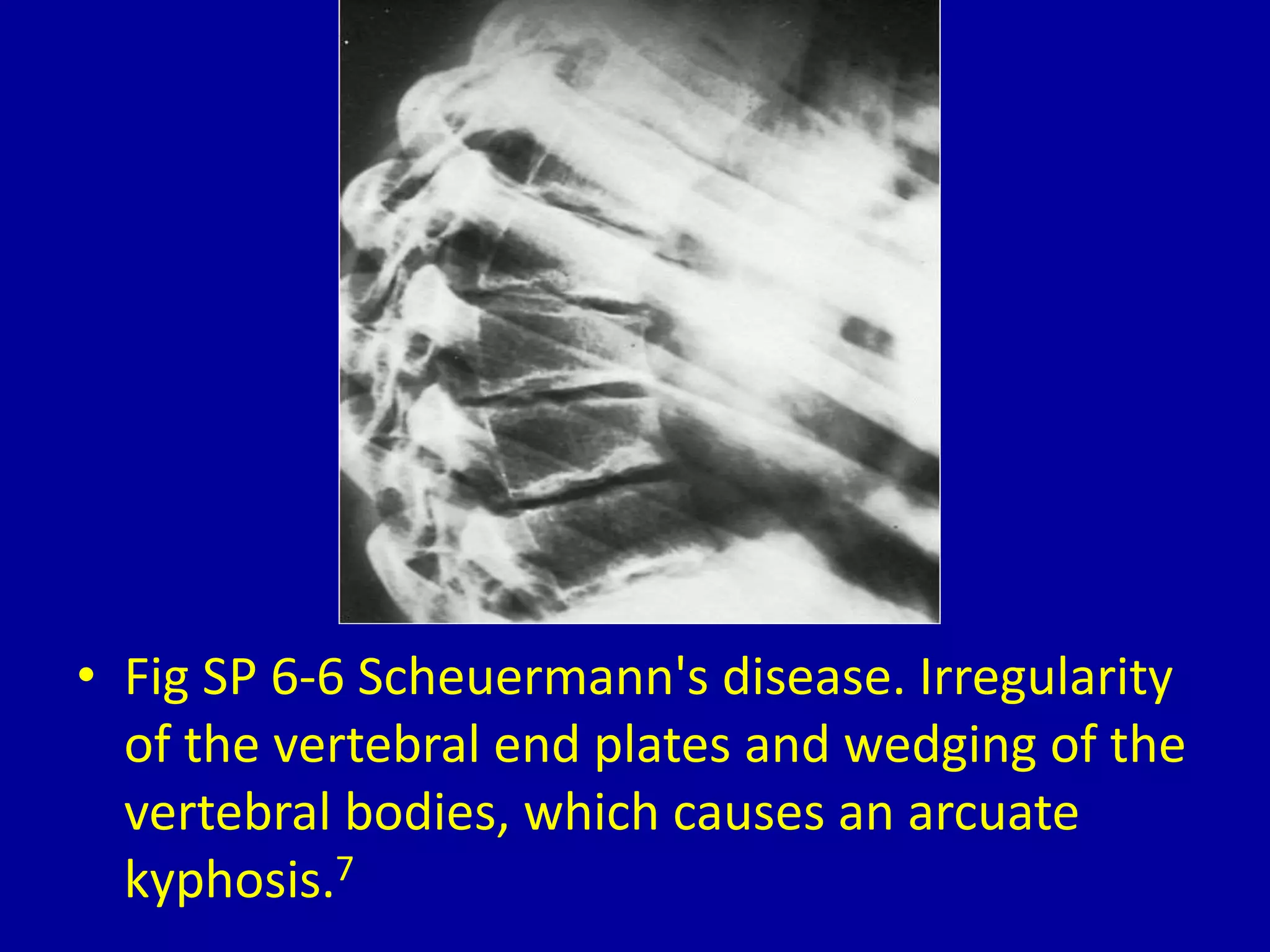
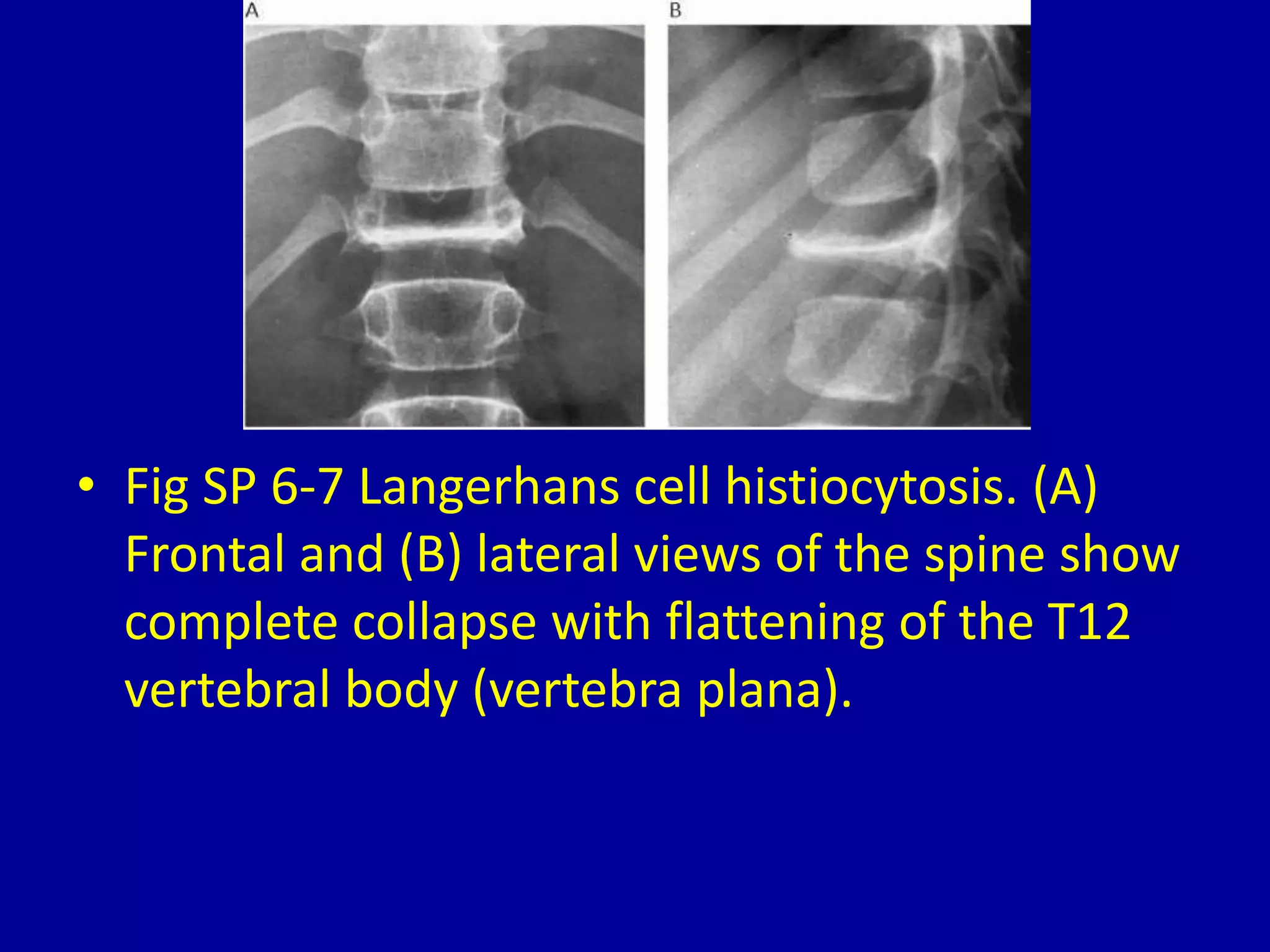
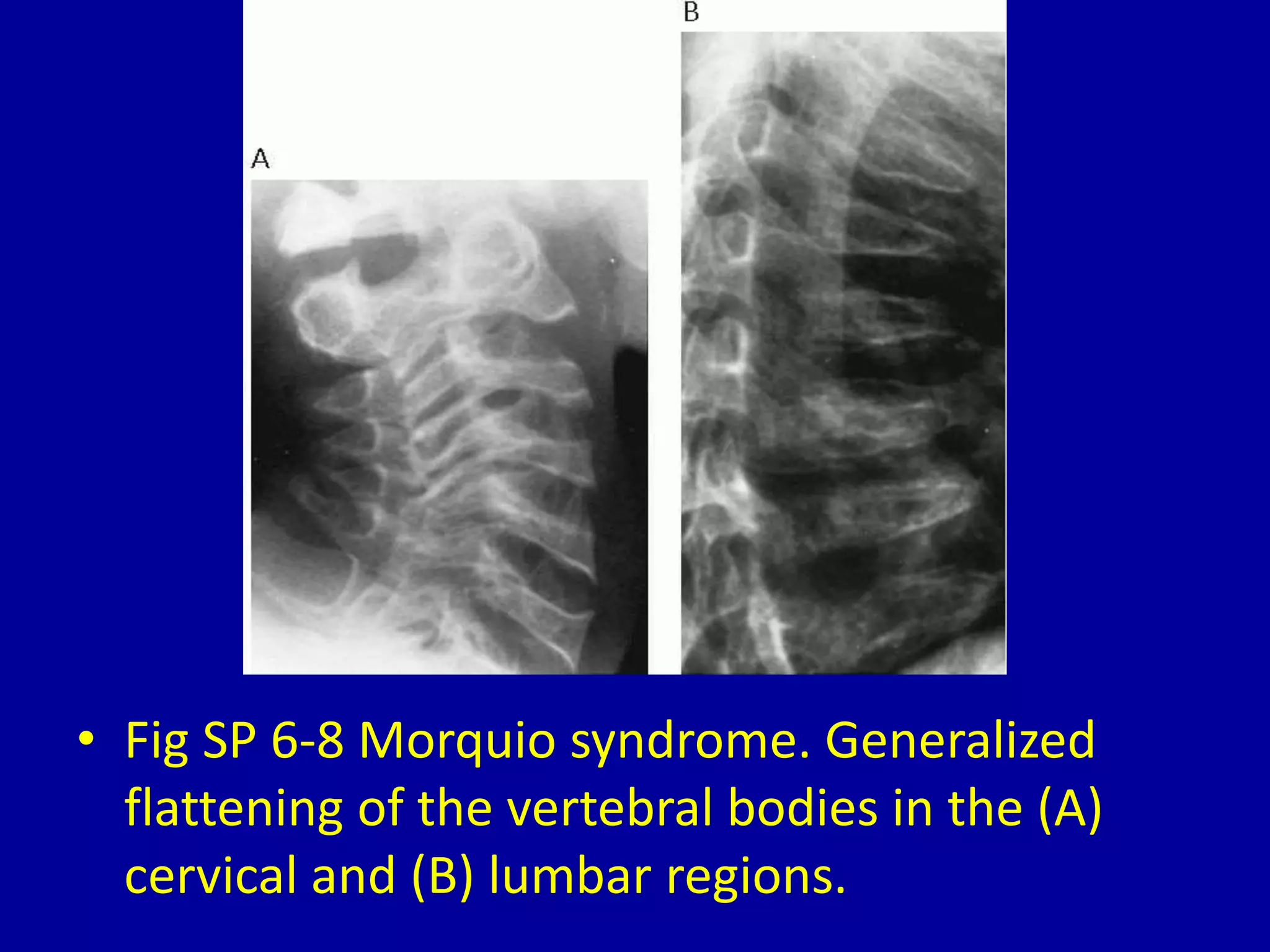


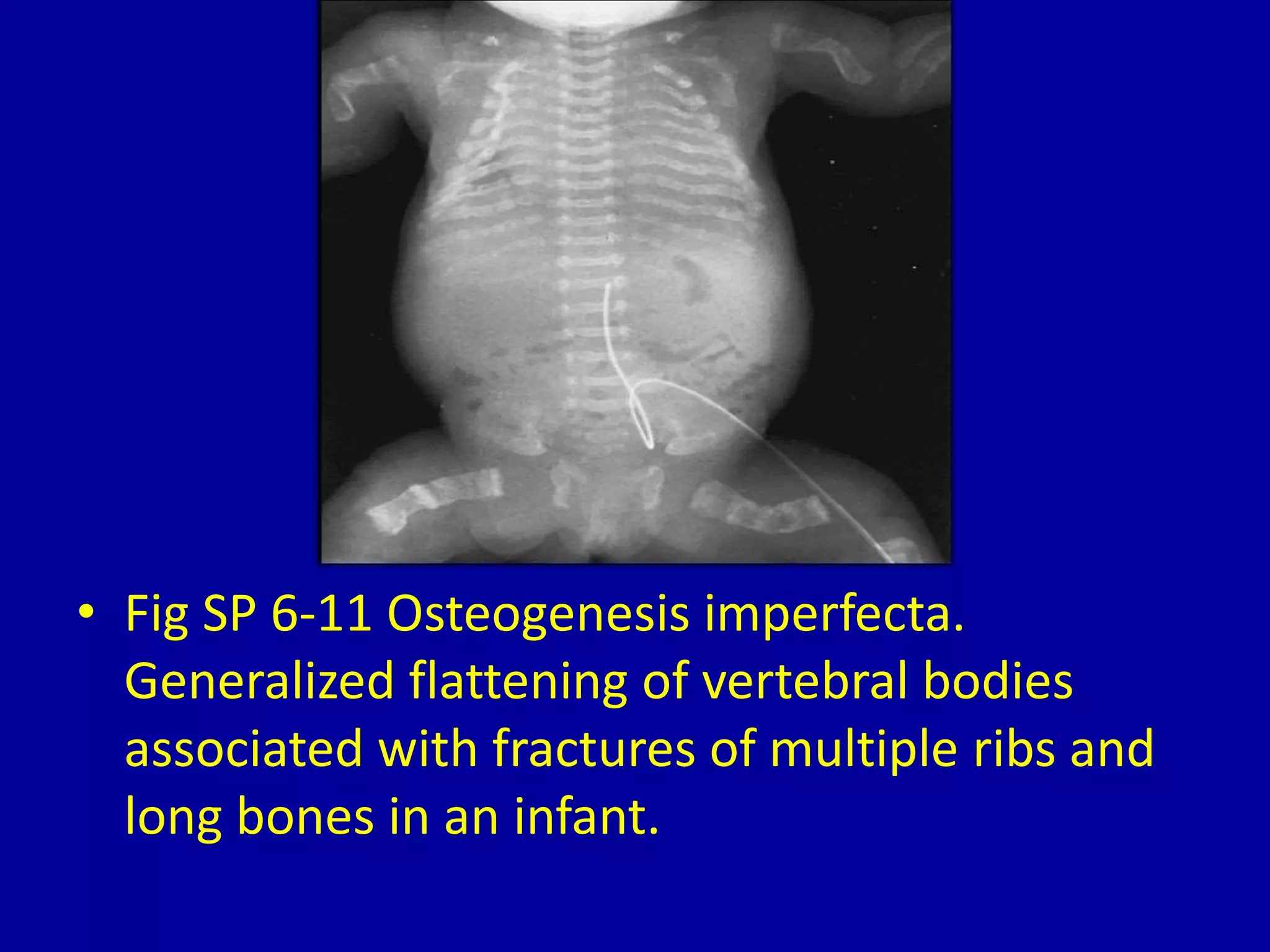




This document discusses loss of height or collapse of one or more vertebral bodies, which can be caused by several conditions. It provides 10 figures showing examples of vertebral body collapse or loss of height due to severe osteoporosis, multiple myeloma, tuberculous osteomyelitis, brucellosis, fracture, Scheuermann's disease, Langerhans cell histiocytosis, Morquio syndrome, spondyloepiphyseal dysplasia, sickle cell anemia, and osteogenesis imperfecta. Each figure illustrates the characteristic radiographic findings of vertebral body abnormalities associated with each condition.