Downloaded 51 times

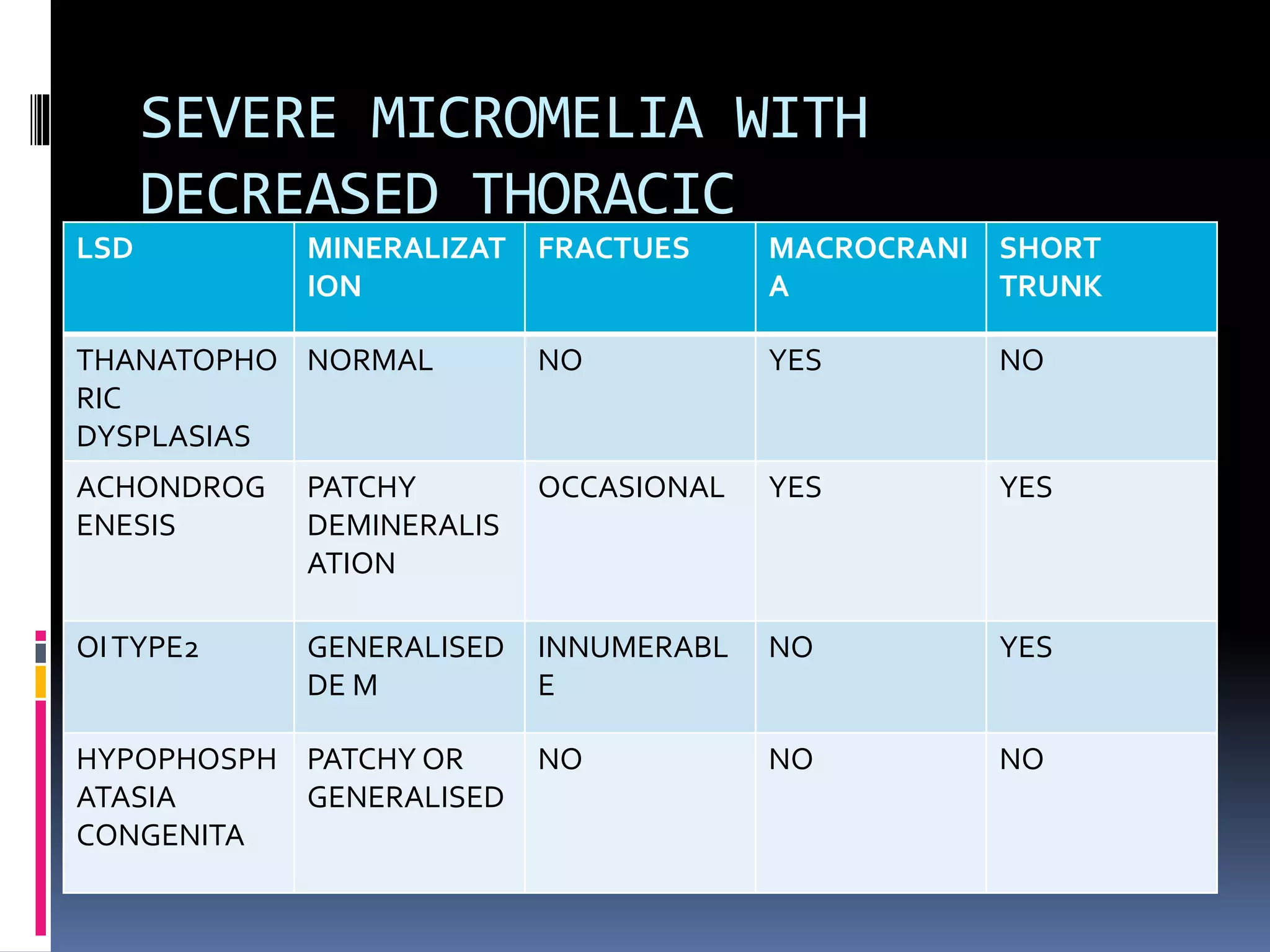










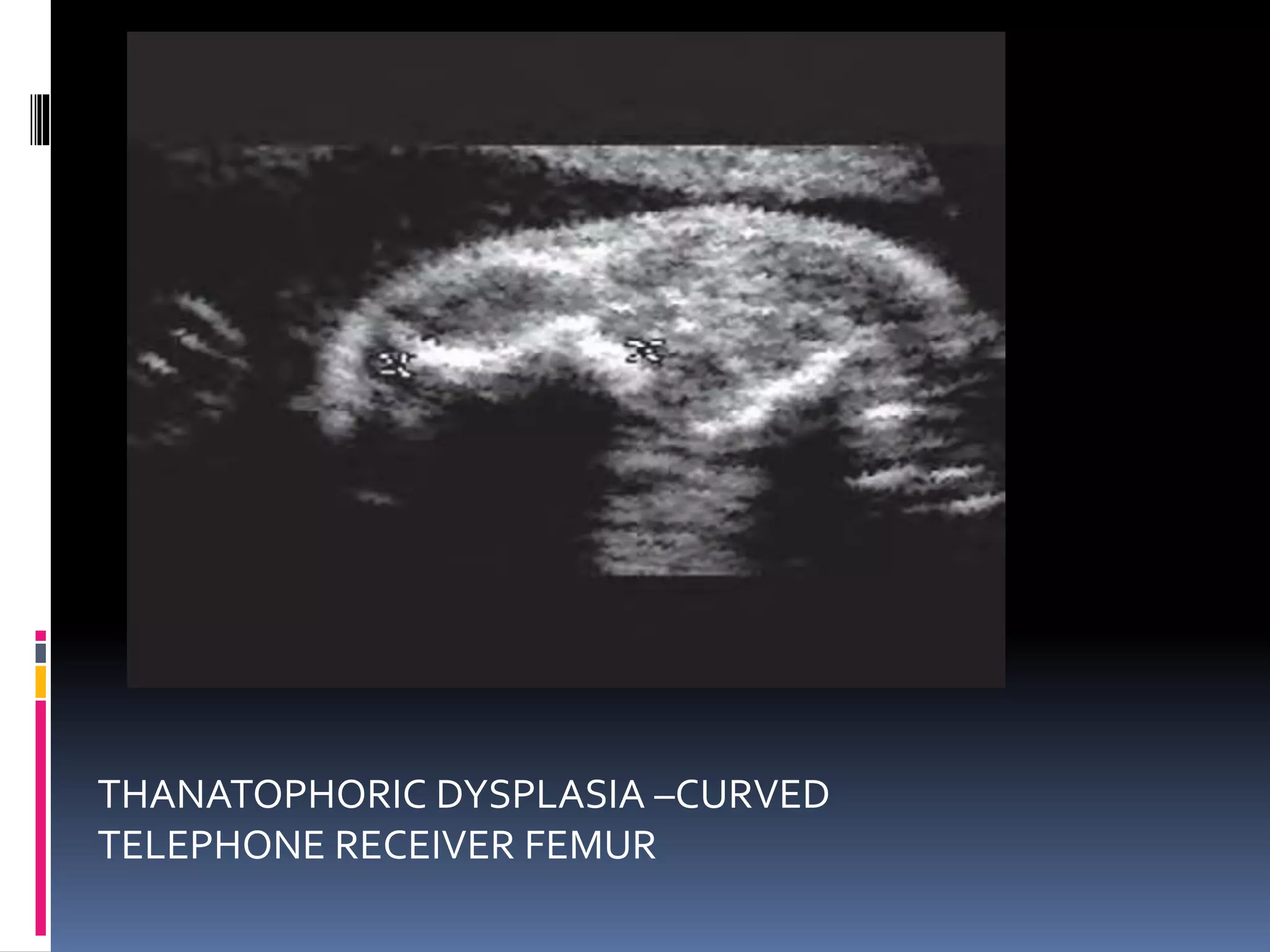
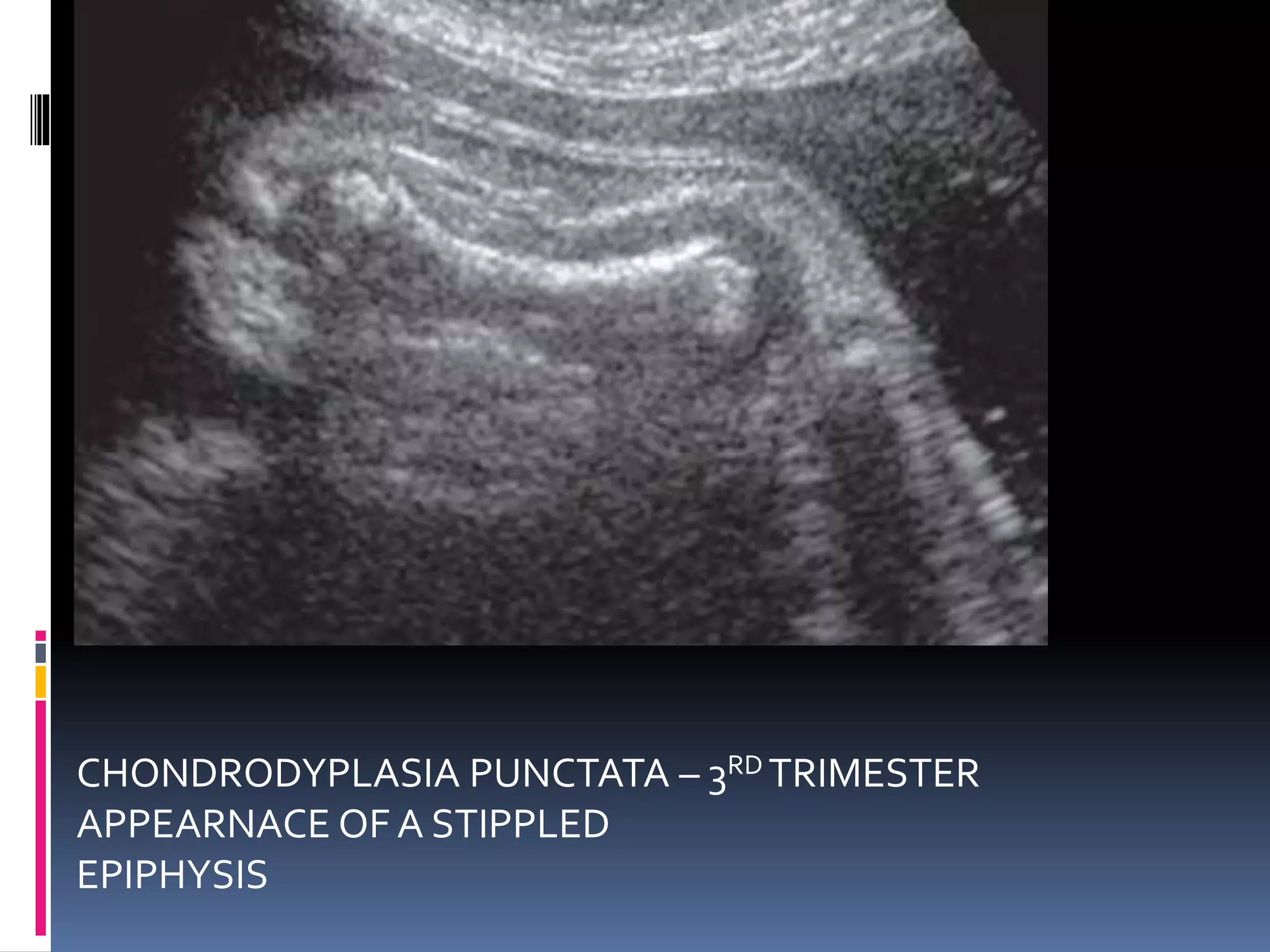
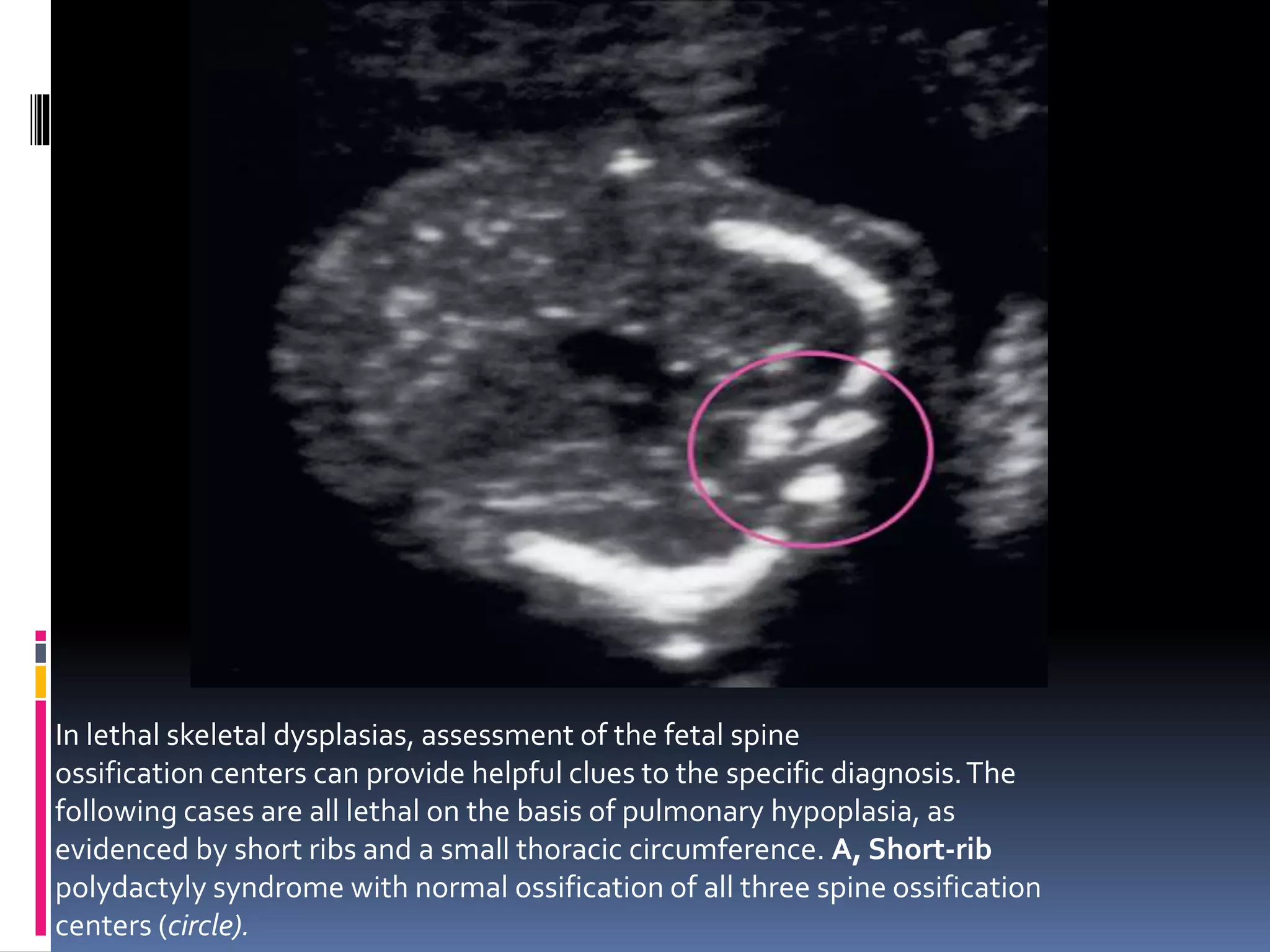
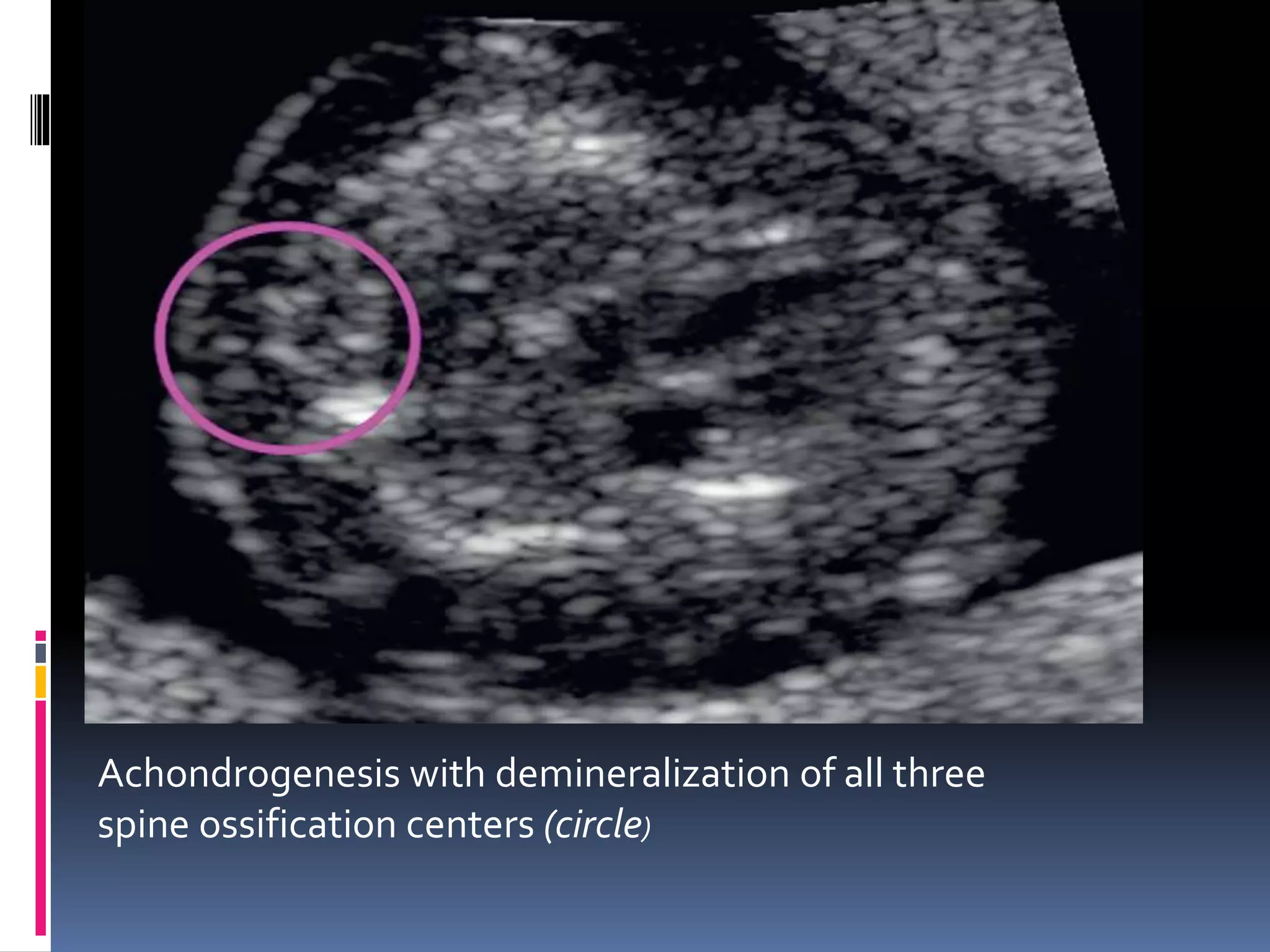


























The document discusses lethal skeletal dysplasias in fetuses, detailing diagnostic features, classifications, and associated conditions such as thanatophoric dysplasia, achondrogenesis, and osteogenesis imperfecta type 2. Key indicators of these conditions include severe micromelia, pulmonary hypoplasia, abnormal mineralization, and specific limb shortening patterns that can be assessed via ultrasound. It emphasizes the significance of early detection in determining prognosis and outlines the typical sonographic hallmarks related to various skeletal dysplasias.