Downloaded 2,066 times











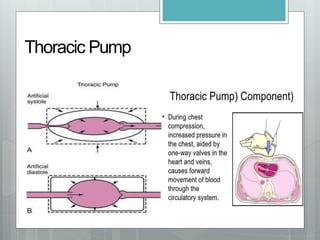



































This document provides information on basic life support (BLS). It begins by defining cardiac arrest as the cessation of normal blood circulation due to heart failure. It describes reversible causes of cardiac arrest including pulmonary embolism, tension pneumothorax, and various toxins or electrolyte imbalances. The basics of BLS are then outlined, including chest compressions, opening the airway, rescue breathing, and defibrillation. Steps of BLS like assessing the scene, checking for breathing and pulse are explained. Chest compression techniques, rescue breathing methods like mouth-to-mouth and bag valve mask, and use of an automated external defibrillator are described. Finally, drugs commonly used in cardiac arrest like epinephrine























































































