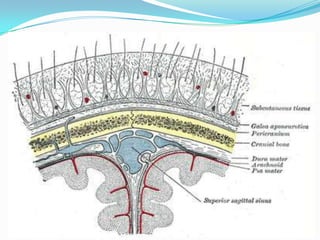
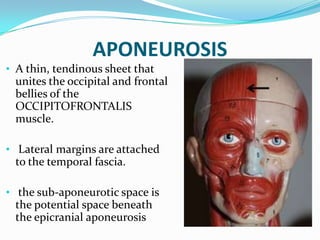
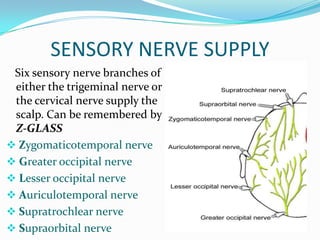
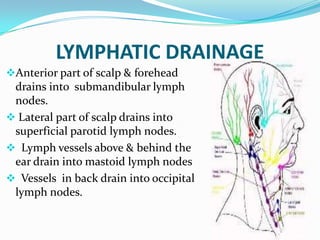
The scalp consists of 5 layers - skin, connective tissue, aponeurosis, loose areolar tissue, and pericranium. The clinically important layer is the aponeurosis, as lacerations through this layer can cause gaping of the wound requiring suturing. The scalp receives innervation from the trigeminal and cervical nerves and is supplied by the supratrochlear, supraorbital, zygomaticotemporal, auriculotemporal, lesser occipital, and greater occipital nerves.