Downloaded 876 times
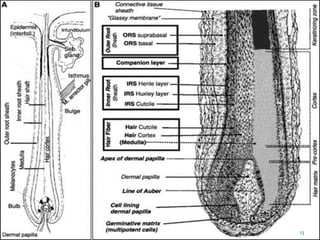
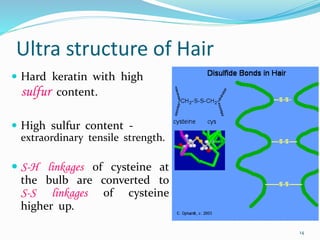
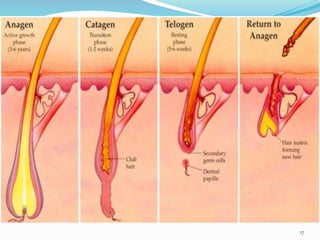
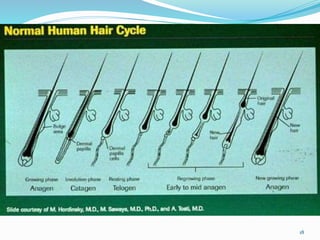
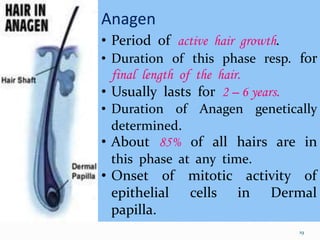
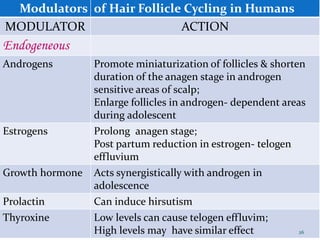
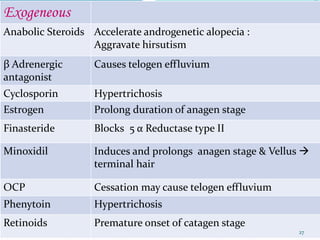
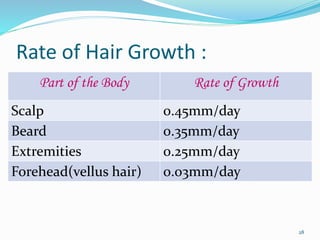
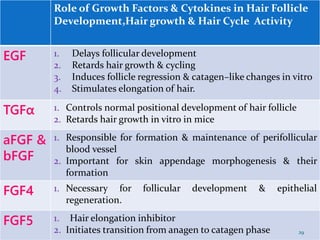
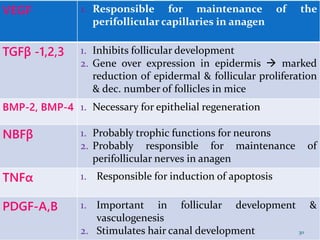
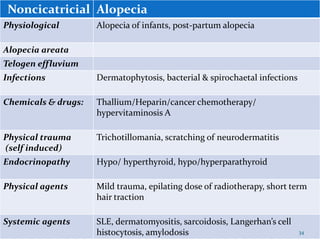
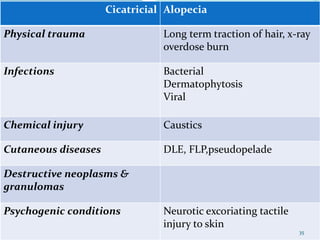
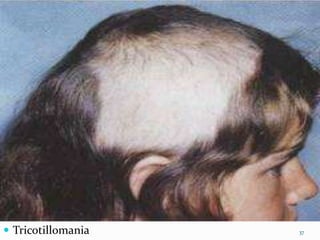
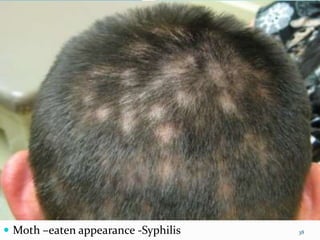




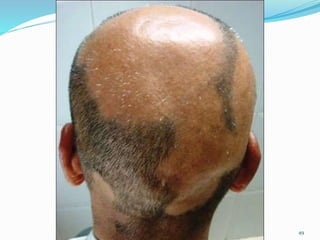




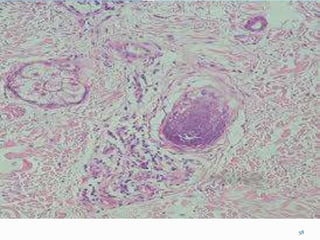
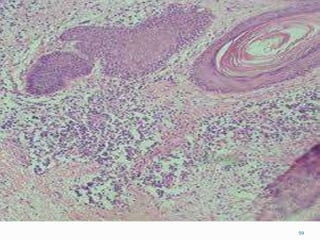
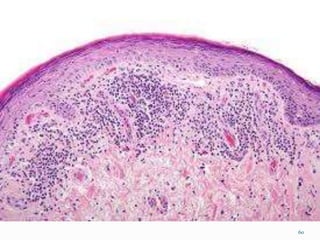
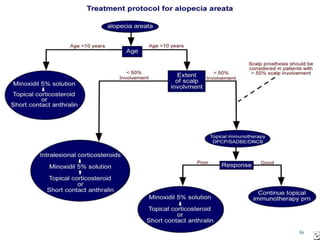
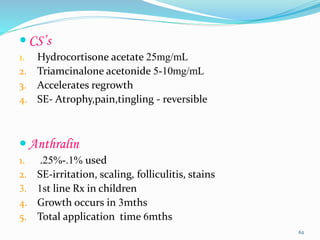
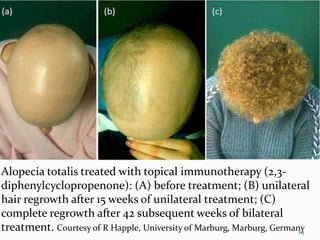
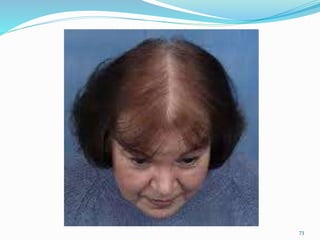
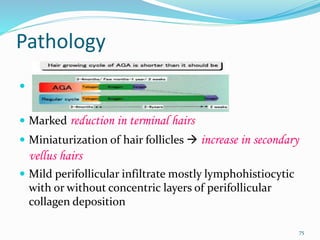
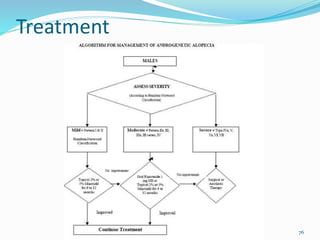
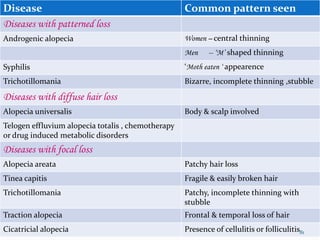
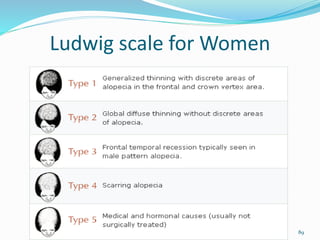



This document discusses hair science and the classification of alopecia. It begins by covering hair anatomy and the hair cycle process. It then classifies different types of alopecia as either noncicatricial (non-scarring) or cicatricial (scarring). One type covered in detail is alopecia areata, which is described as a chronic inflammatory disorder characterized by patchy hair loss without scalp atrophy. The etiology, clinical features, investigations, histopathology and prognosis of alopecia areata are summarized.



































































