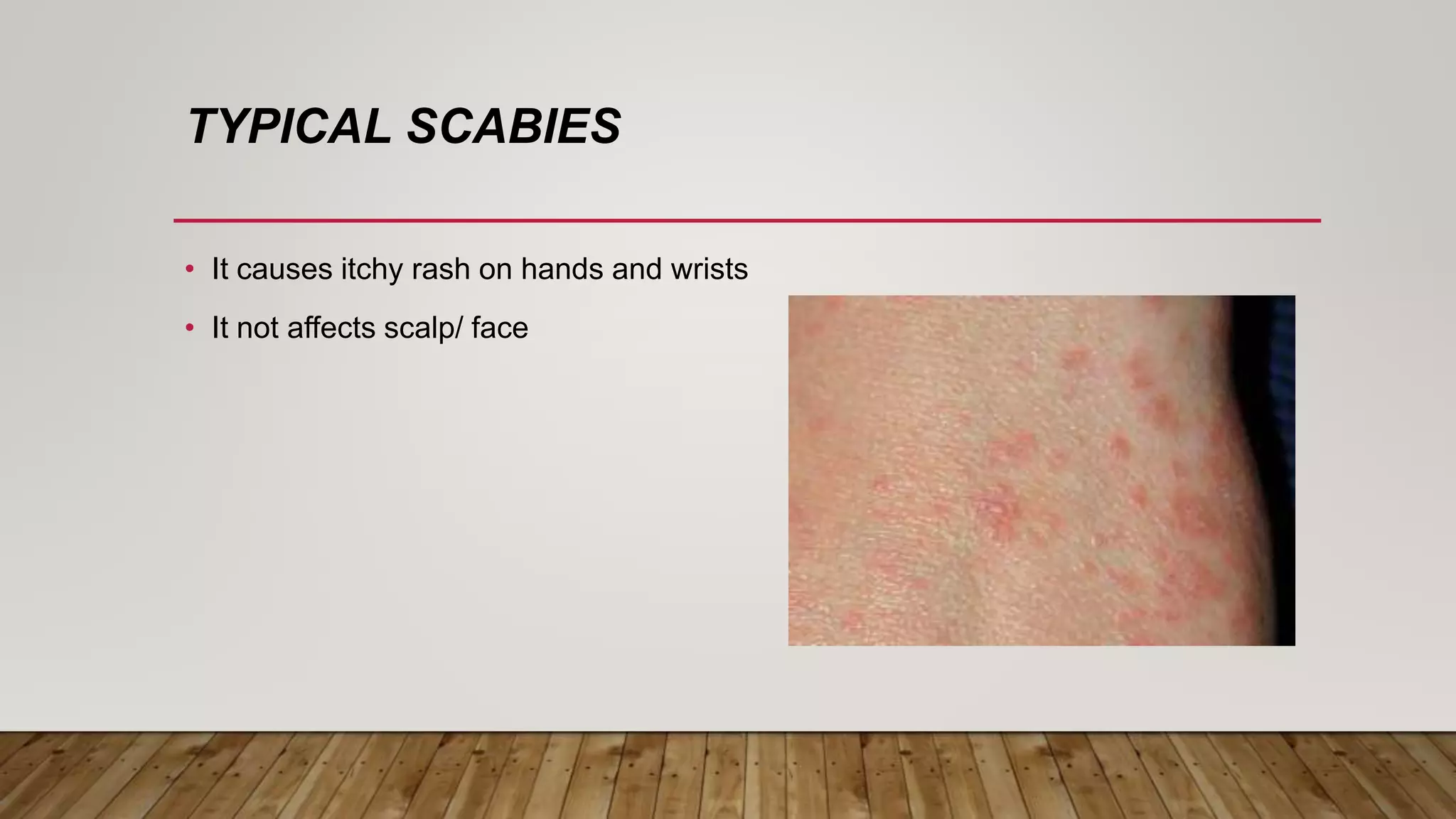
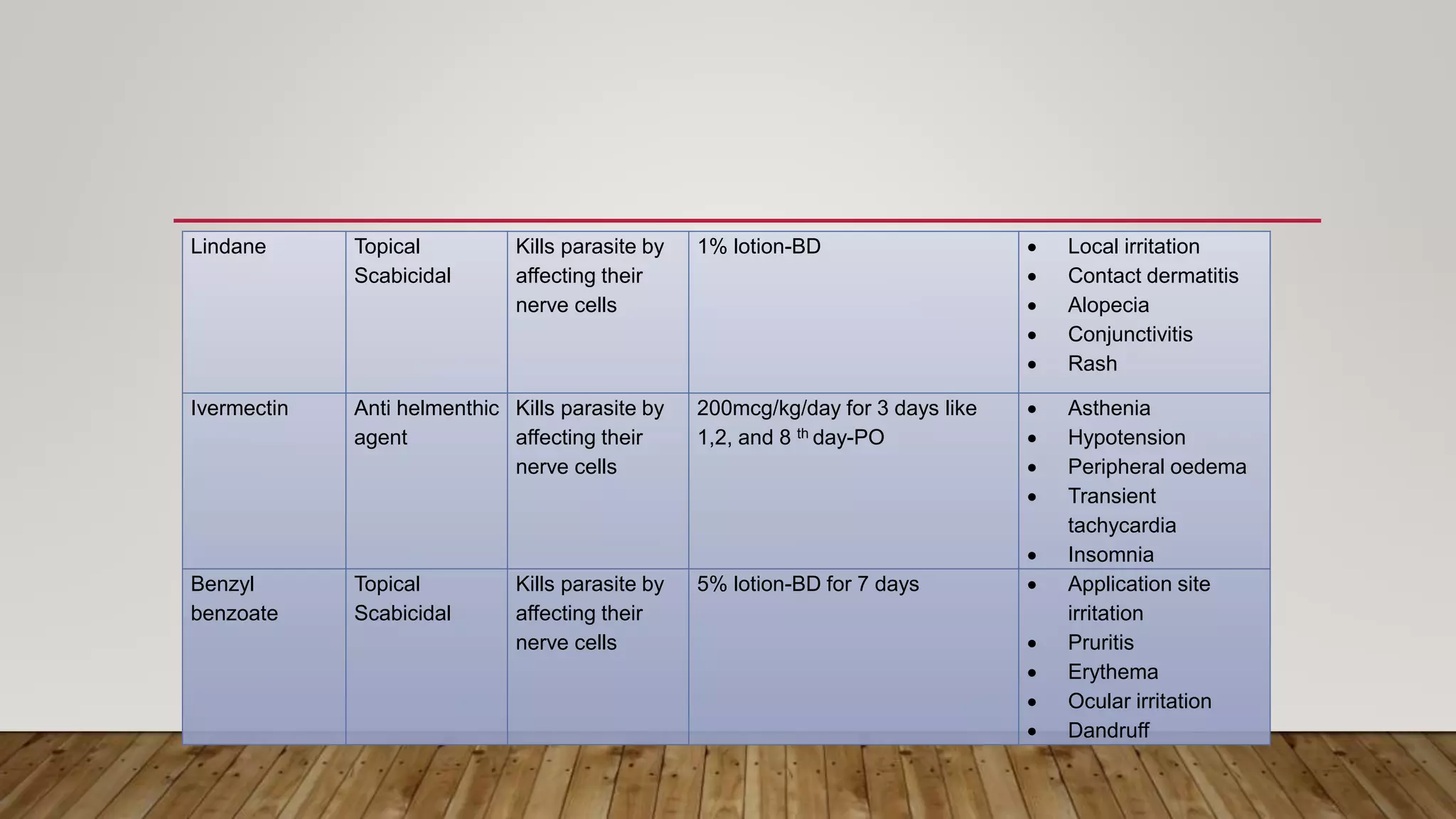
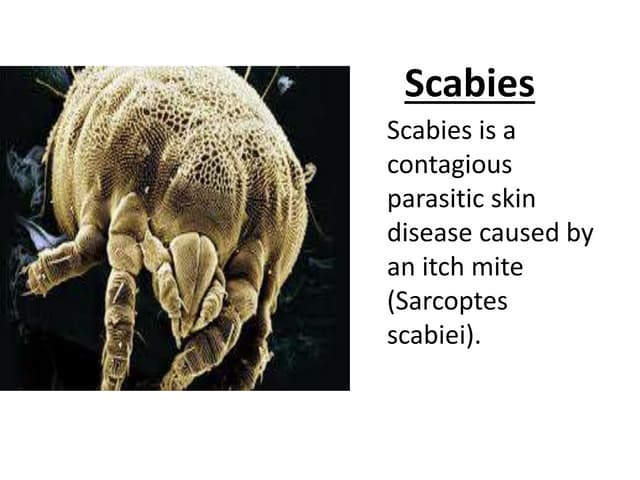
Scabies is a skin infection caused by the Sarcoptes scabiei mite. It causes an itchy rash and affects nearly 130 million people worldwide, with prevalence rates in India ranging from 13-59% in rural and urban areas respectively. Scabies presents as itchy papules and vesicles located typically on hands, wrists, feet, and genitalia. It can develop into more severe forms like nodular or crusted scabies in immunocompromised individuals. Treatment involves topical scabicides like permethrin or oral ivermectin. Proper hygiene and avoiding shared items can help prevent transmission.
























































![Scabies [Derma] smol.pptxbees bees bees bees](https://cdn.slidesharecdn.com/ss_thumbnails/scabiesdermasmol-241012052828-db33758e-thumbnail.jpg?width=640&height=640&fit=bounds)










































