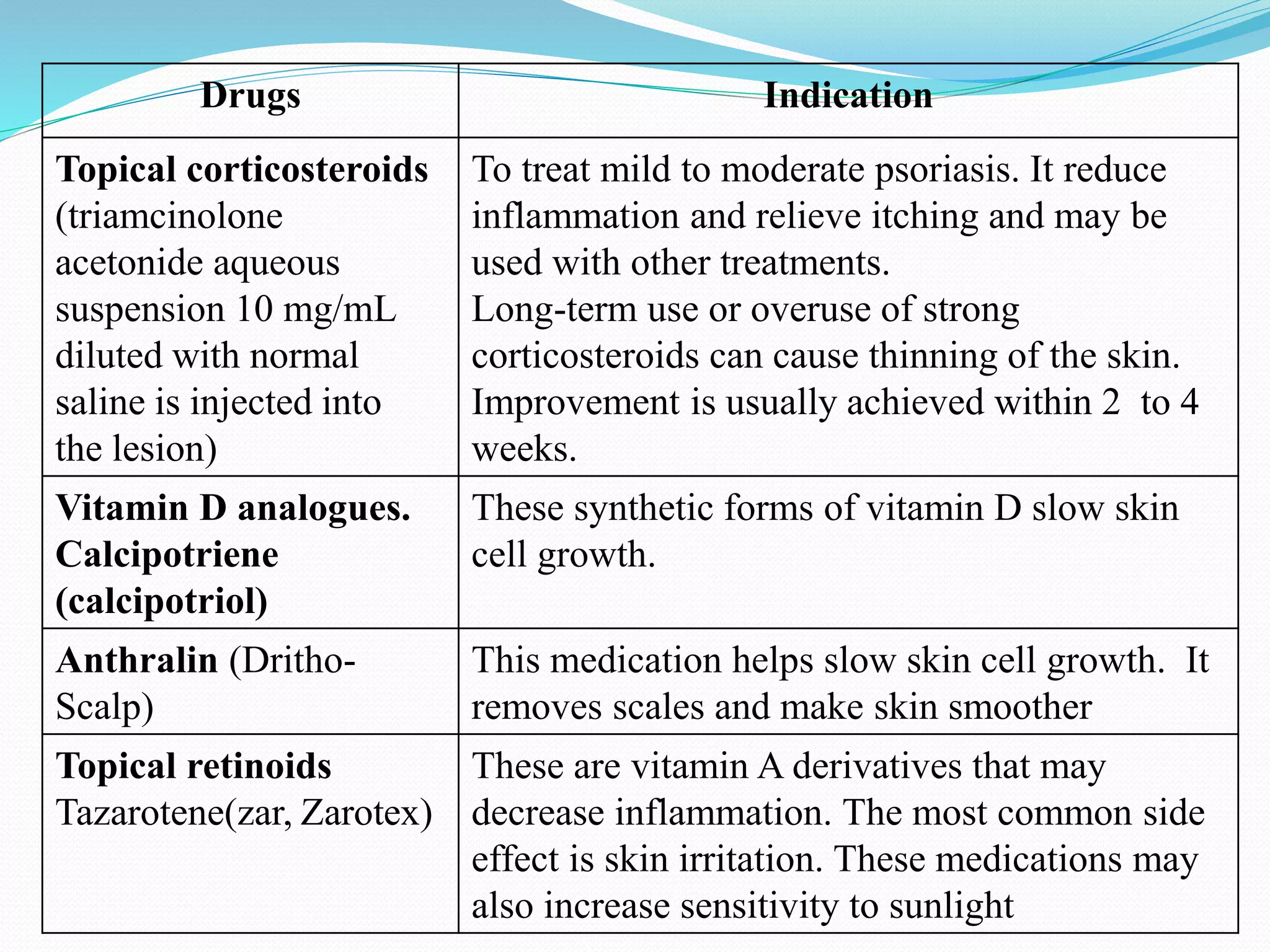
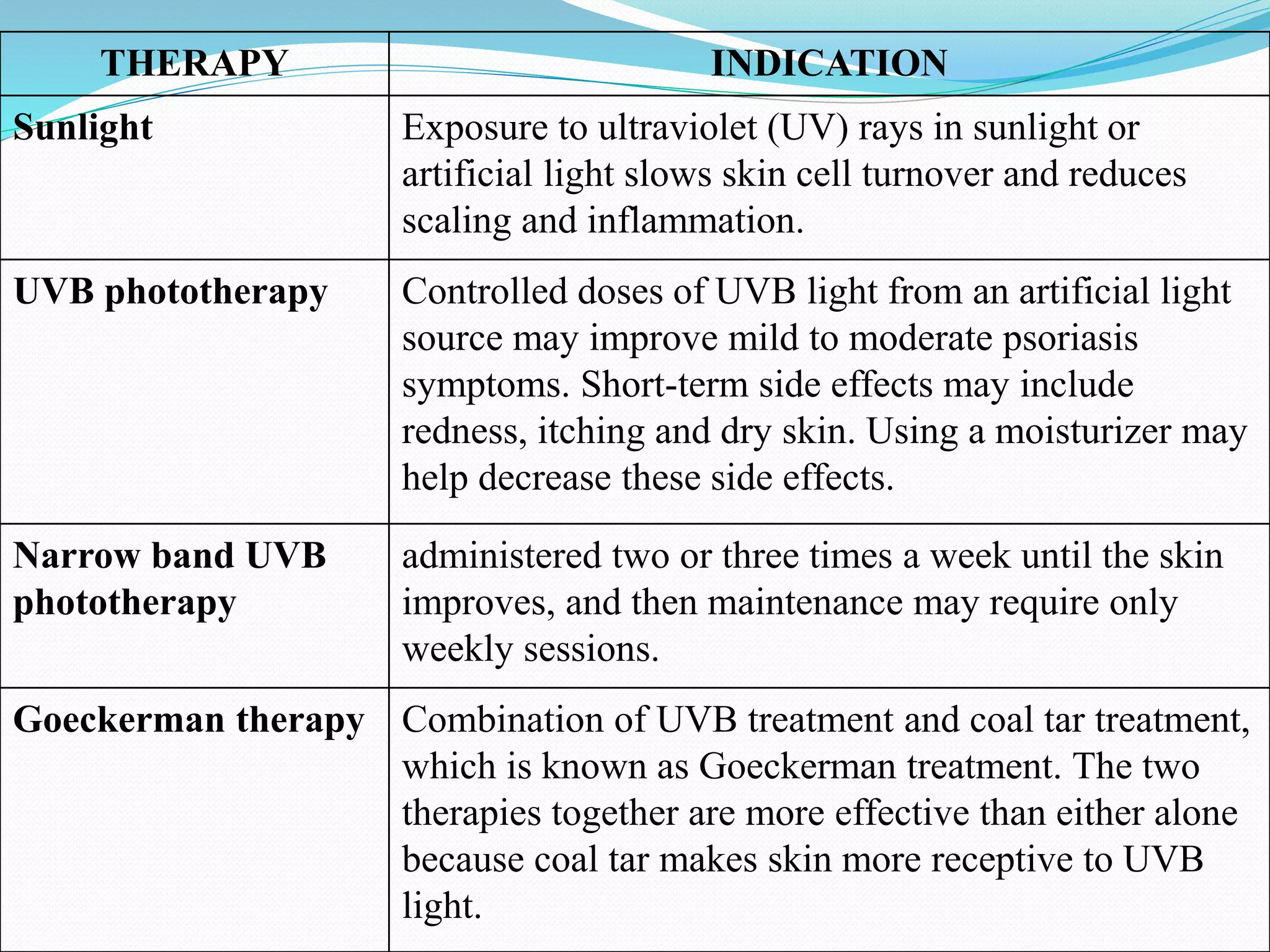
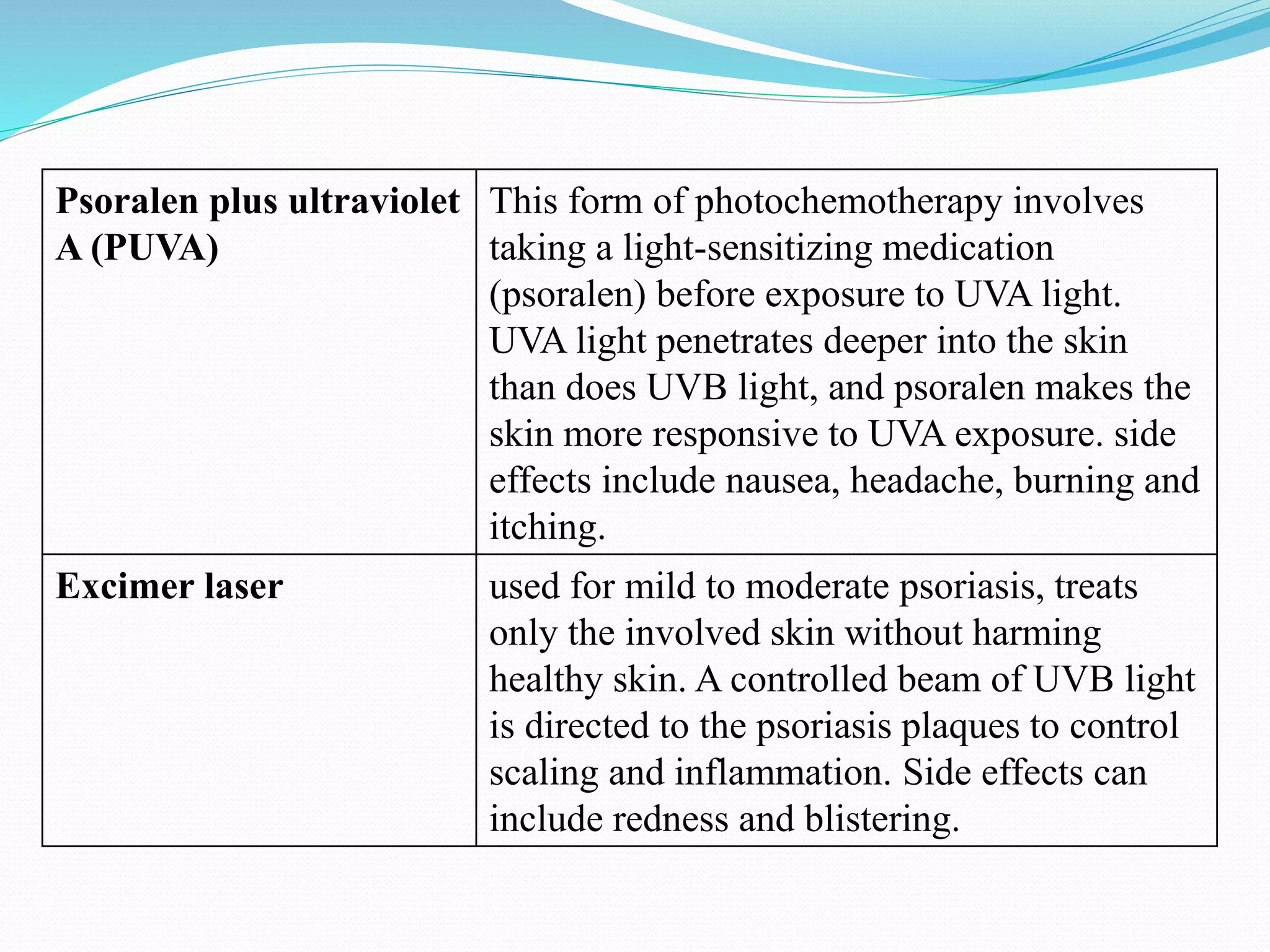
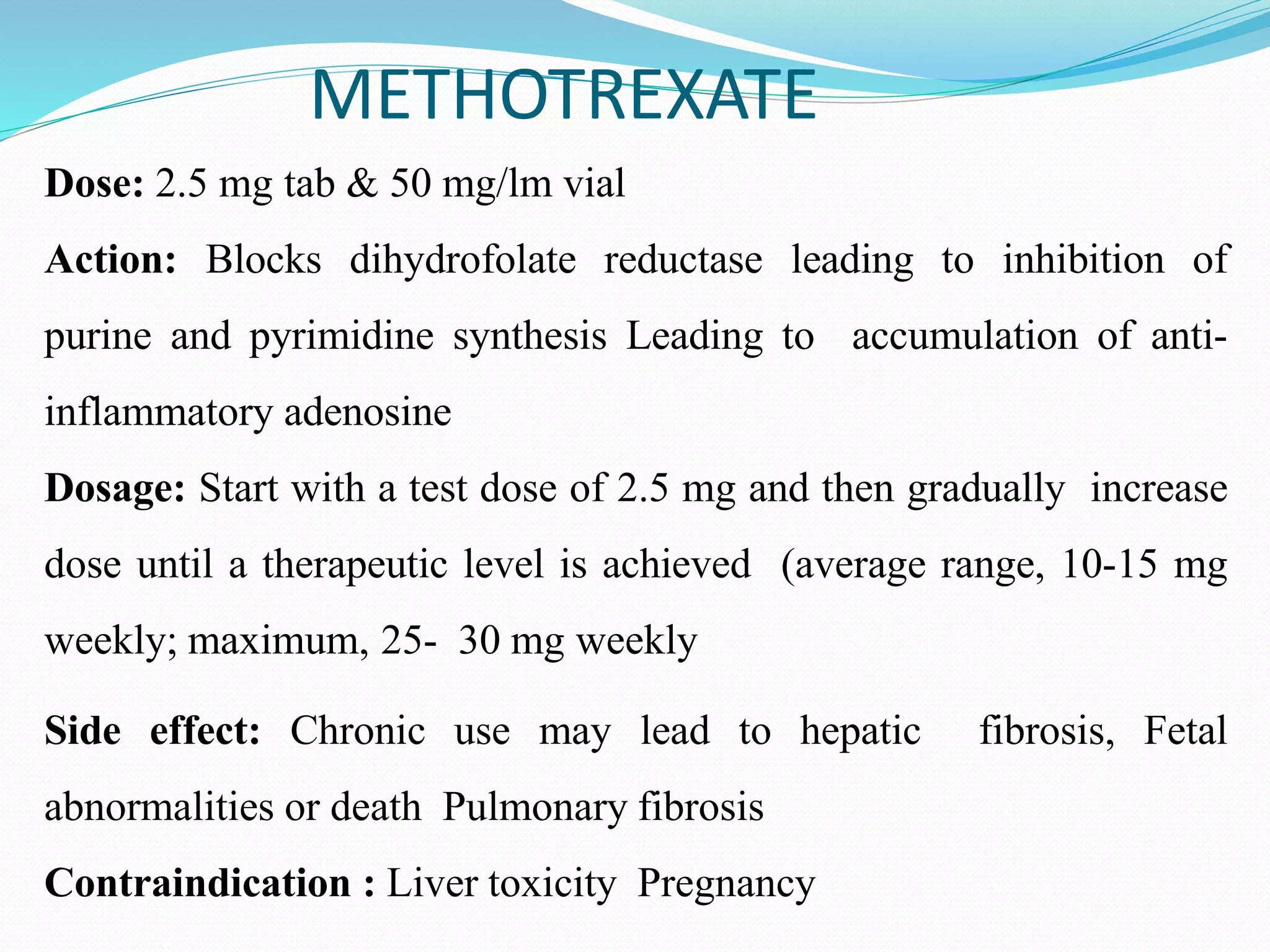
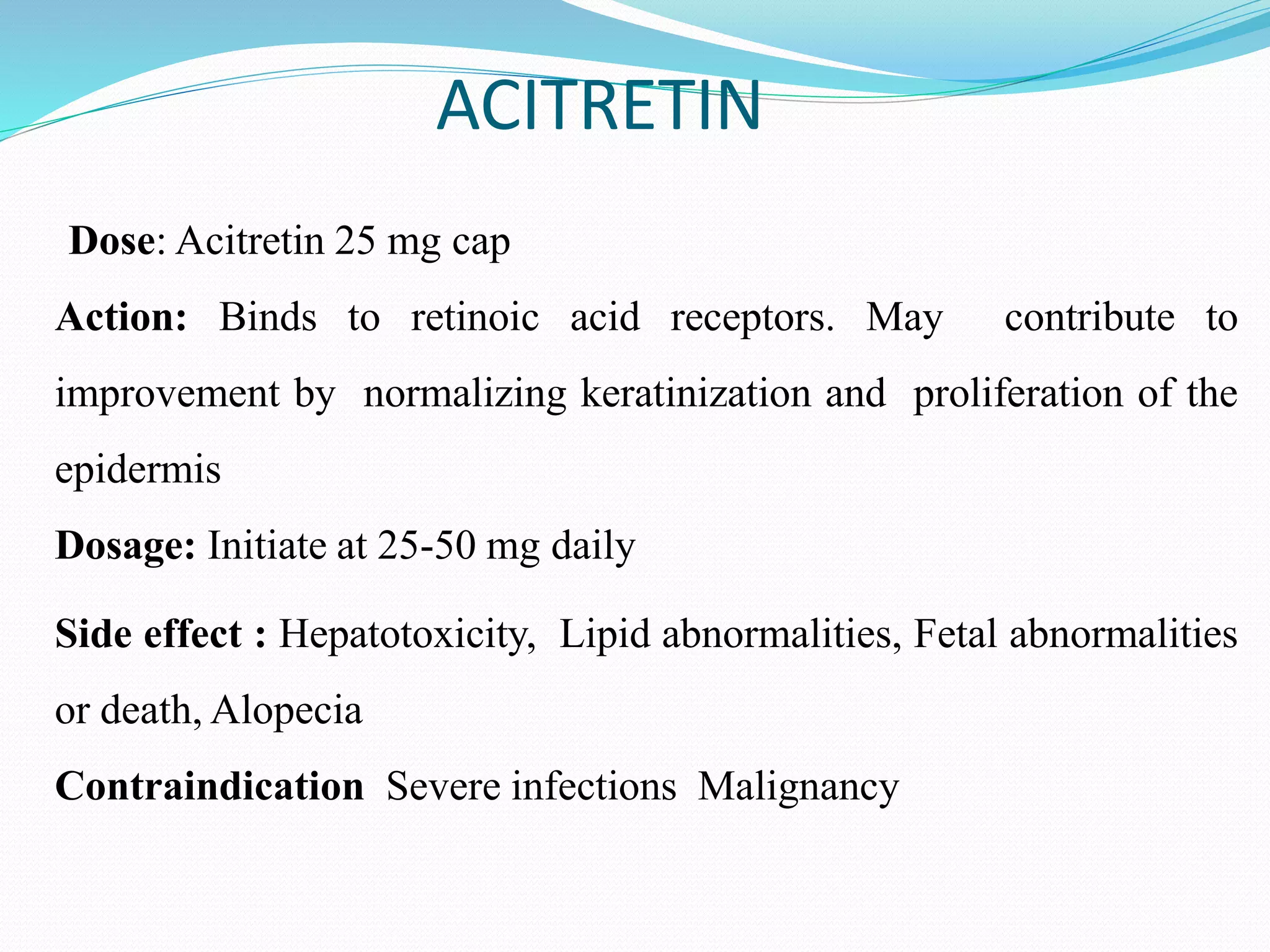
Psoriasis is a chronic, inflammatory skin condition characterized by thickened patches of red skin covered by silvery scales. It occurs when the immune system causes skin cells to grow too quickly. The document defines psoriasis and describes the main types, risk factors, diagnosis, and treatment options including topical therapies, phototherapy, and systemic medications that target the immune system. Treatment aims to reduce inflammation and scaling based on the severity and location of symptoms.