Downloaded 195 times

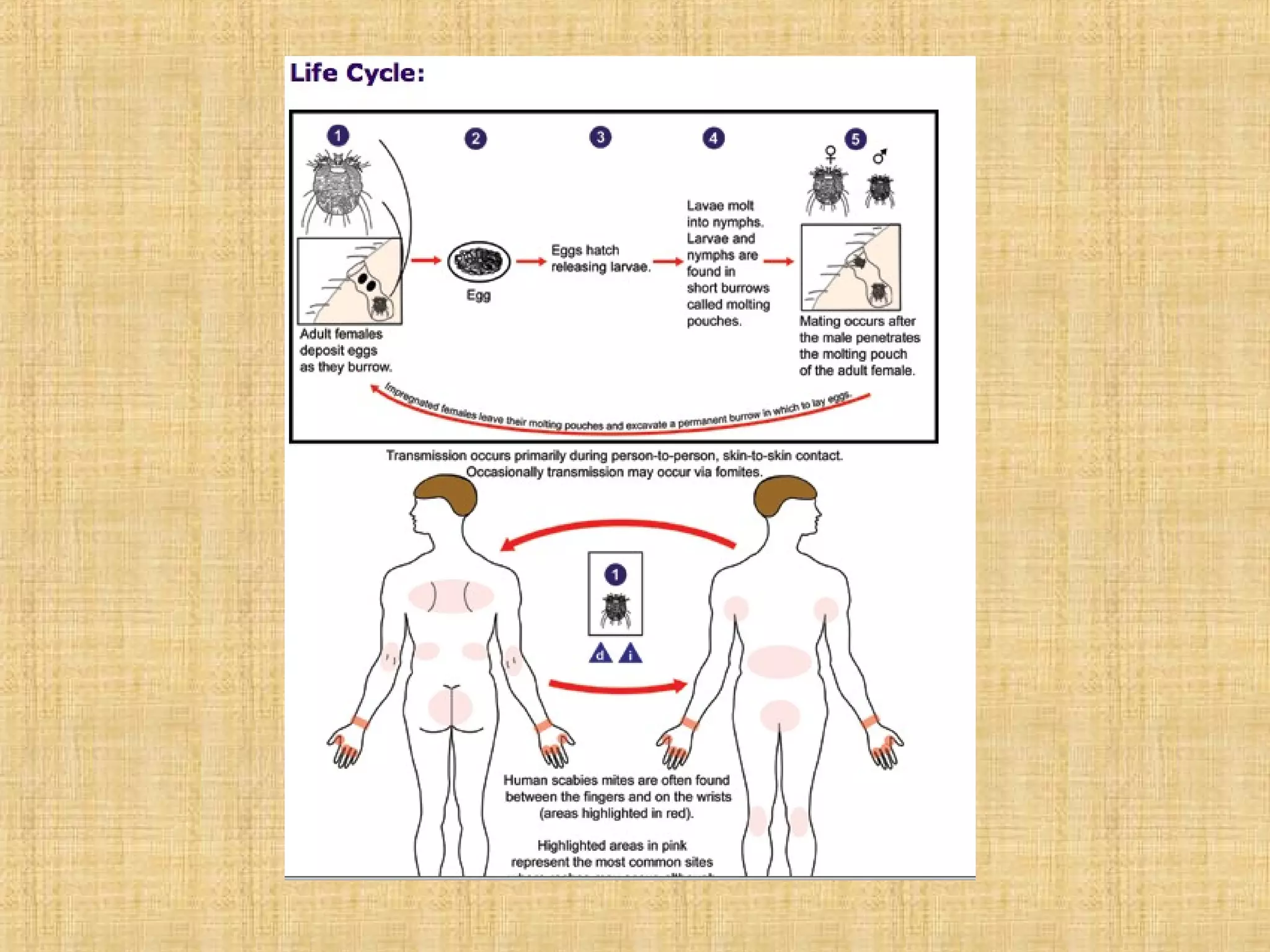
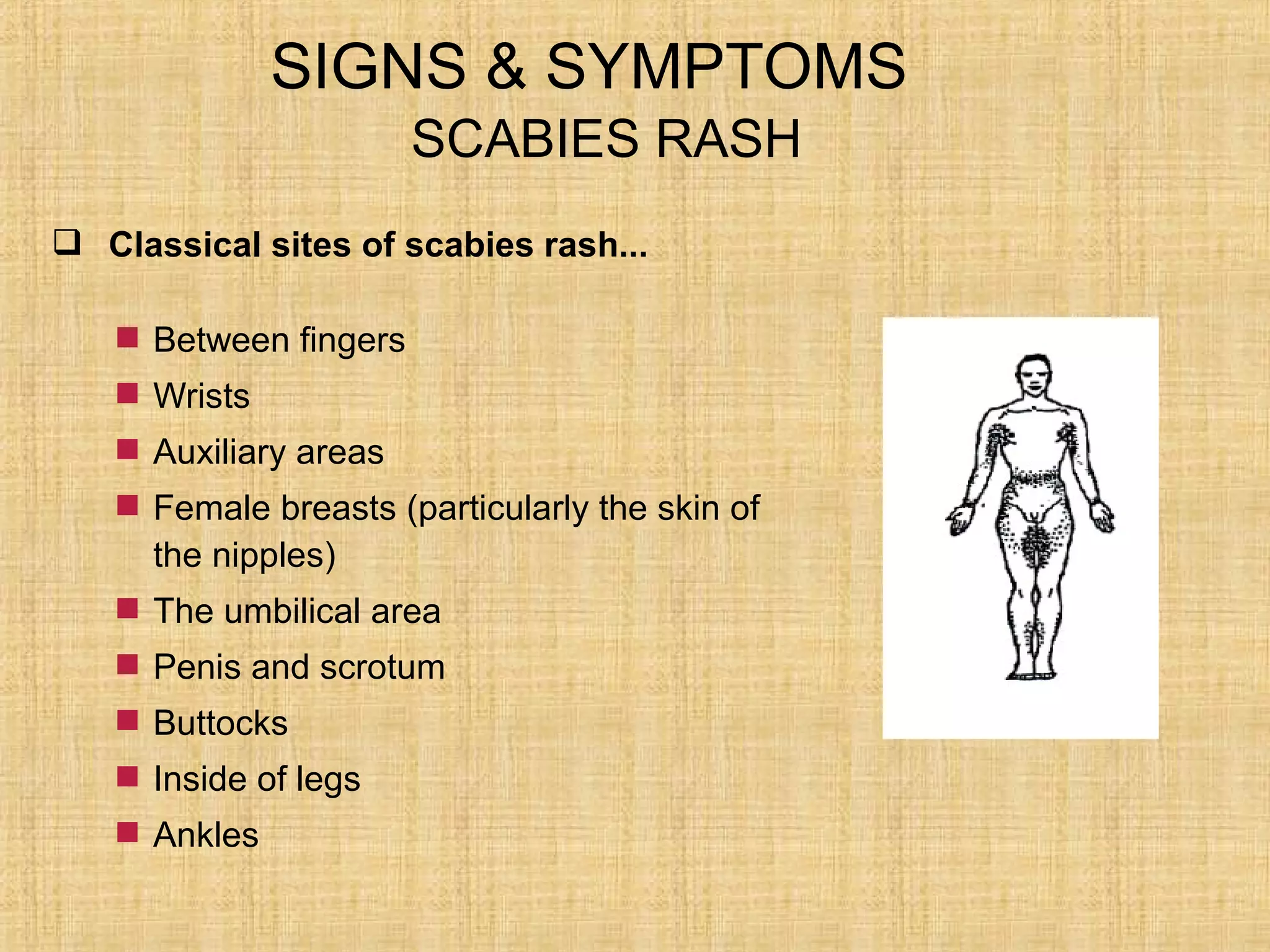





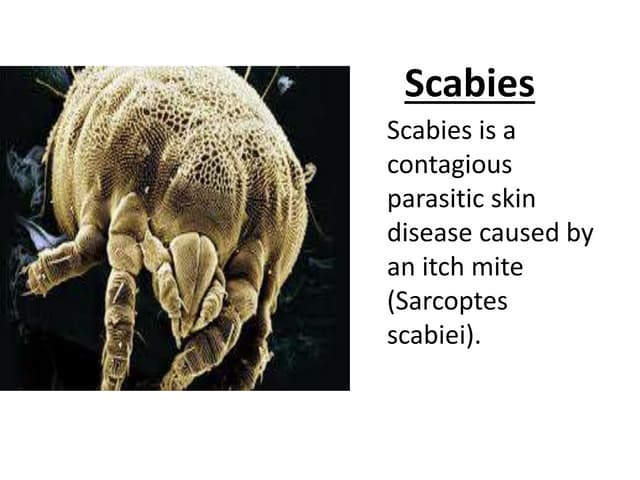
Scabies is a contagious skin disease caused by tiny mites called Sarcoptes Scabiei. It is transmitted through direct skin-to-skin contact or contact with infected clothing or bedding. Symptoms include a pimple-like rash that usually appears between fingers, wrists, breasts, genitals, buttocks, and ankles. Diagnosis involves identifying mites, eggs or feces under microscopy of skin scrapings. Treatment involves applying a scabicide cream or lotion like permethrin or ivermectin all over the body from the neck down and washing all clothing and bedding. Prevention requires observing new residents for rashes and maintaining vigilance for und





















































![Scabies [Derma] smol.pptxbees bees bees bees](https://cdn.slidesharecdn.com/ss_thumbnails/scabiesdermasmol-241012052828-db33758e-thumbnail.jpg?width=640&height=640&fit=bounds)


























