Downloaded 131 times

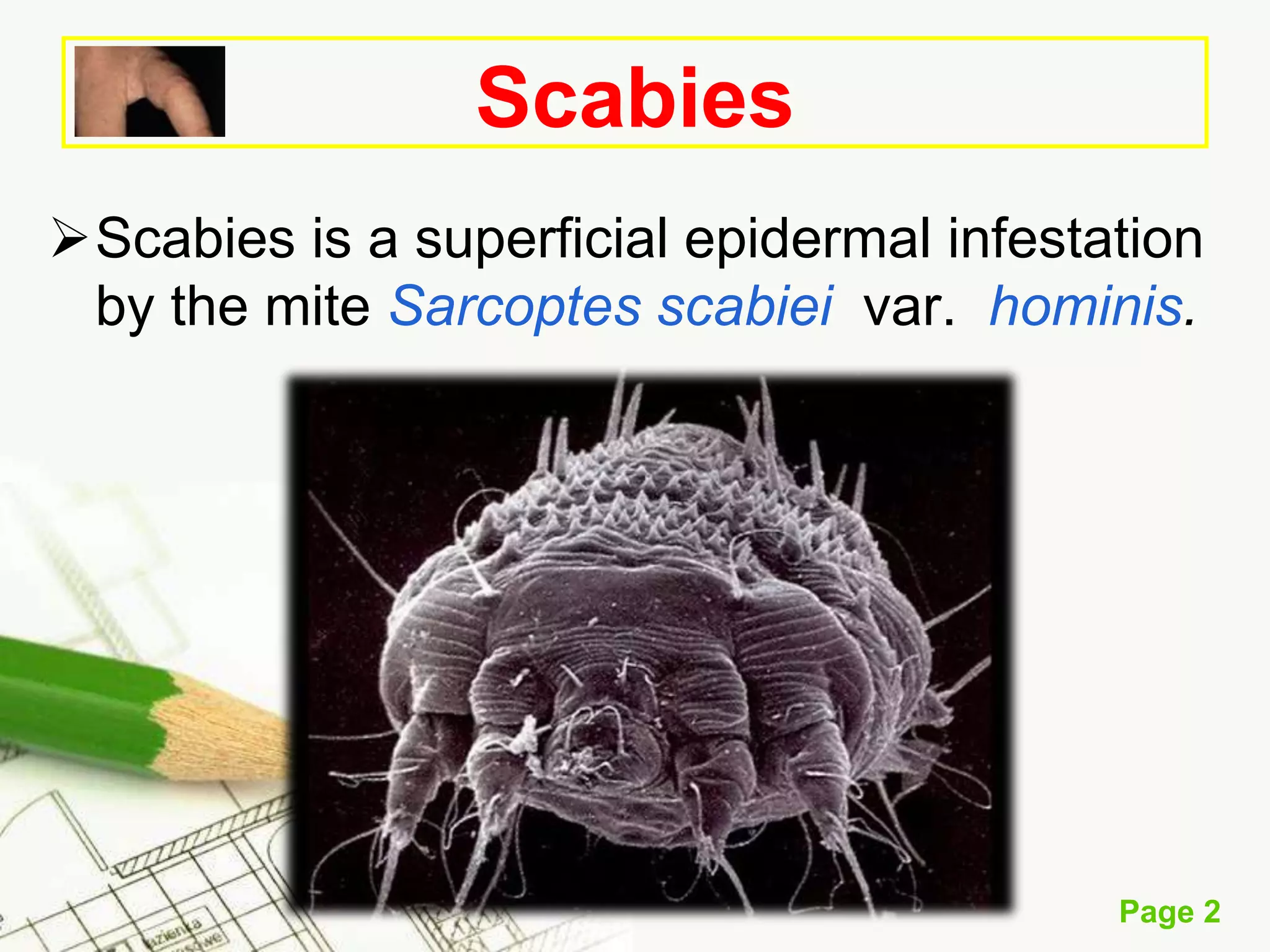





















Scabies is a skin infestation caused by the mite Sarcoptes scabiei var. hominis, commonly affecting children and individuals in care facilities, transmitted primarily through skin-to-skin contact and fomites. Clinical symptoms include pruritus and characteristic lesions, with varying incubation periods for initial and reinfestation, and can lead to secondary bacterial infections. Effective management includes the use of topical scabicides like permethrin and lindane, as well as systemic treatments for severe cases.











































![Scabies [Derma] smol.pptxbees bees bees bees](https://cdn.slidesharecdn.com/ss_thumbnails/scabiesdermasmol-241012052828-db33758e-thumbnail.jpg?width=640&height=640&fit=bounds)


































