Downloaded 408 times
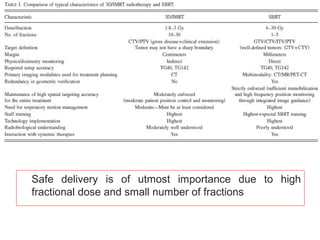
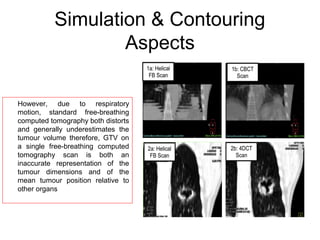
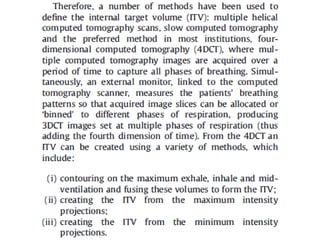
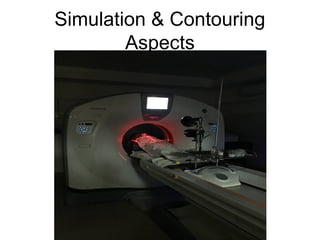

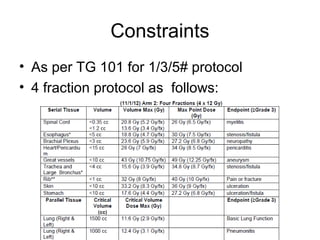
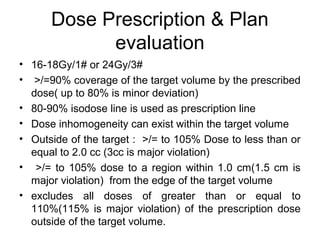
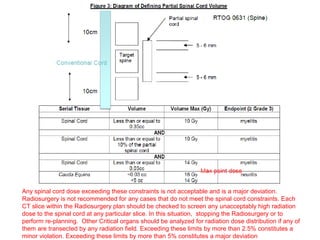
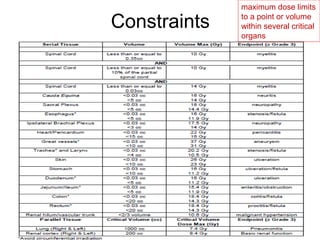
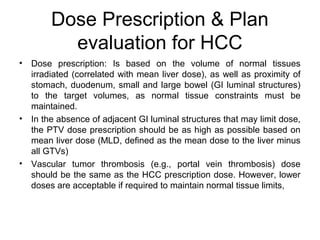
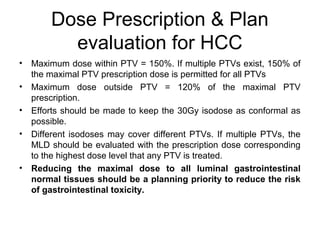
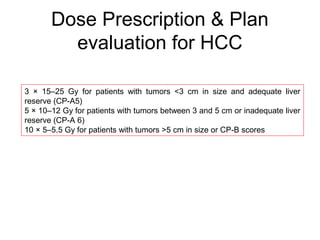
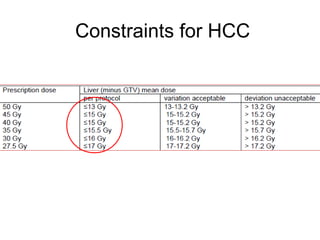



This document provides contouring and treatment planning guidelines for stereotactic body radiation therapy (SBRT). It discusses indications, contraindications, simulation, target volume delineation, organ at risk contouring, dose prescription, and plan evaluation for SBRT treatment of lung, spine, liver, and other cancers. Key considerations include ensuring accurate tumor targeting given organ motion, minimizing dose to nearby organs at risk, and prescribing ablative doses in a small number of fractions to achieve tumor control.




















































![CASE_PRESENTATION_ON_subdural_hematoma(SDH)[1 FINAL PPT]-1.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/casepresentationonsubduralhematomasdh1finalppt-1-260129172522-d405d375-thumbnail.jpg?width=640&height=640&fit=bounds)














