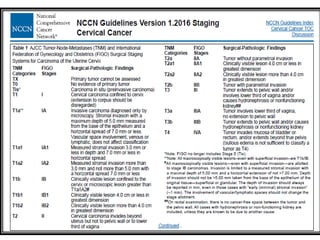
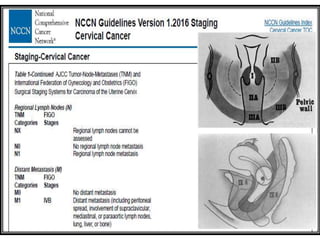
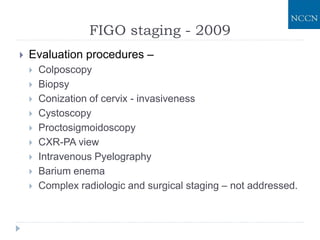
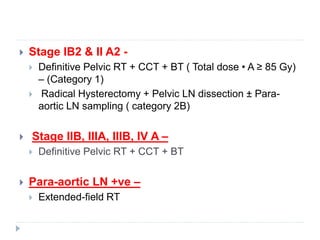
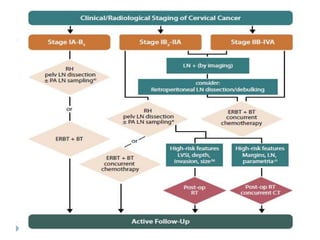
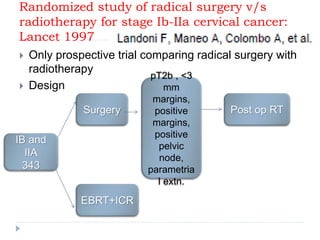
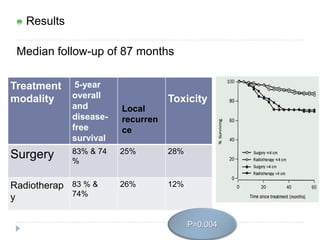
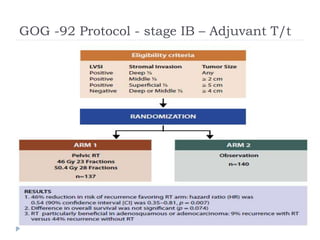
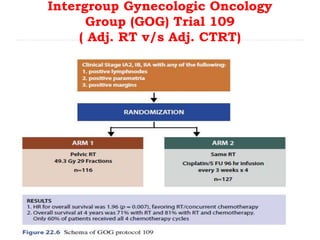
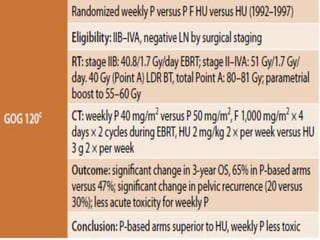
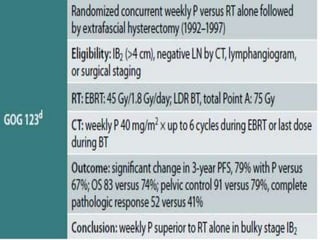
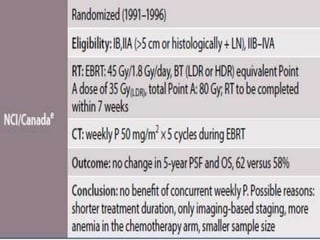
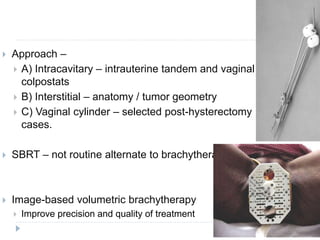
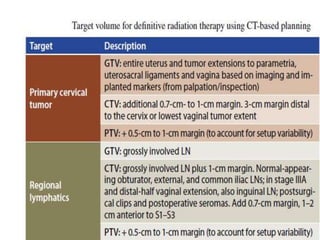
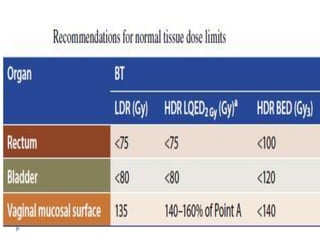
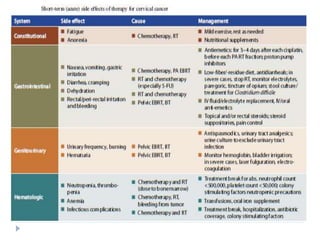
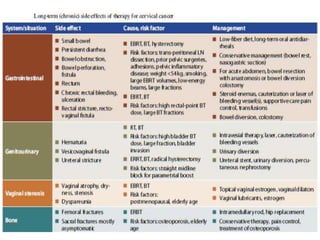
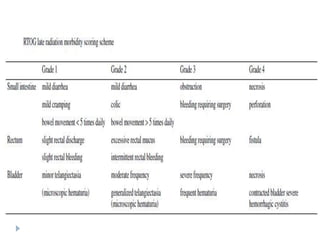
The document discusses the non-surgical management of carcinoma cervix. It describes the FIGO staging system and evaluation procedures. For early stage disease (IA-IB1), options include radical hysterectomy or radiotherapy. For stage IB2-IIA, concurrent chemoradiation is the standard treatment. Brachytherapy is an essential component of definitive treatment and aims to deliver high radiation doses to the cervix and paracervical tissues. Proper radiation treatment planning and adherence to timelines are important to achieve optimal outcomes while minimizing toxicity.






























![Management Of Early Stage Ca Cervix [Autosaved]](https://cdn.slidesharecdn.com/ss_thumbnails/management-of-early-stage-ca-cervix-autosaved-1233338415127954-2-thumbnail.jpg?width=640&height=640&fit=bounds)


























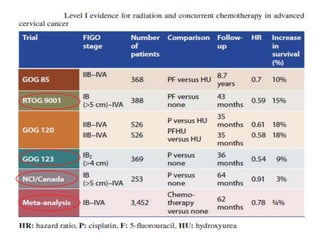
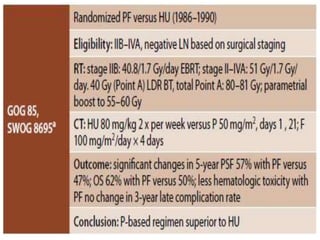
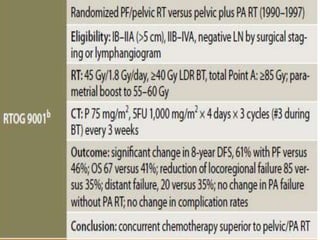
![management of advanced cervical cancer [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/managementofadvancedcervicalcancerautosaved-230926014710-62f747b3-thumbnail.jpg?width=640&height=640&fit=bounds)































