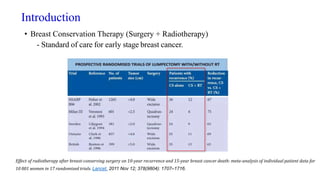
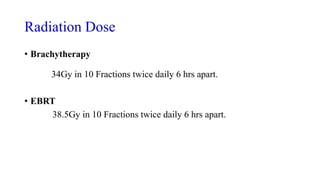
1) Accelerated partial breast irradiation (APBI) delivers radiation to only the portion of the breast surrounding the tumor site after breast-conserving surgery, shortening treatment time compared to whole breast irradiation (WBI).
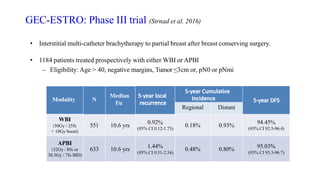
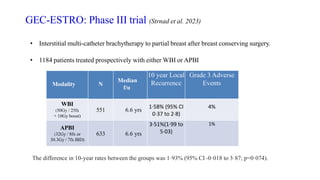
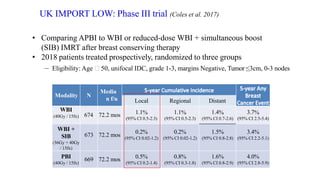
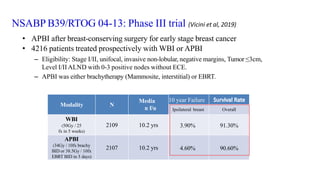
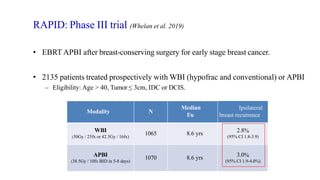
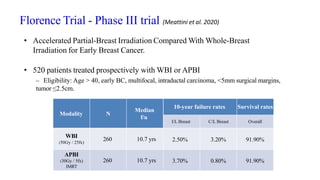
2) Several phase III trials have found APBI to have local control rates comparable to WBI with reduced toxicity, though some trials found slightly higher recurrence rates with APBI.
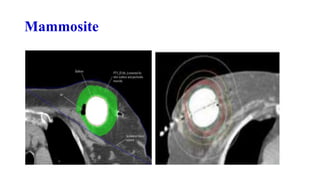
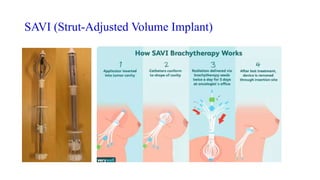
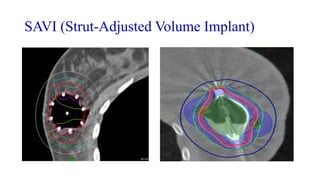
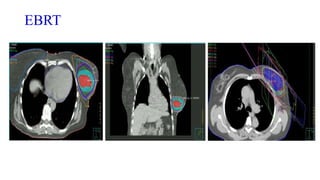
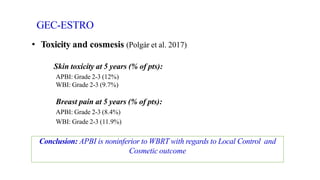
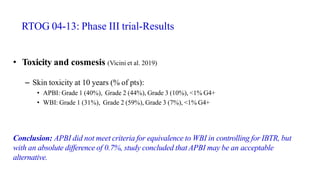
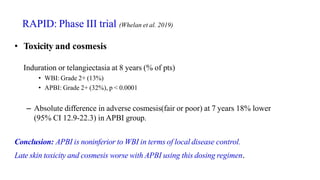
3) Toxicity and cosmetic outcomes vary by technique, with brachytherapy generally showing better results than external beam techniques.