Downloaded 342 times

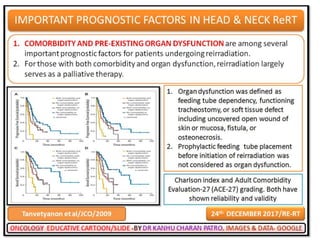

![Imaging-staging
• Biopsy is mandatory.
• The sensitivity and specificity of PET-computed tomography (CT)
for detecting distant metastasis is reported to be 86–91 and 84–
93%, respectively.
• [Gourin CG et.al, Perlow A et.al]
• Re-staging is of paramount importance as up to 25% of patients
will have metastatic disease.
– [Gourin CG et.al, Perlow A et.al]
• MRI demonstrated a trend towards improved sensitivity (96.4 vs
82%) for detecting local recurrence of nasopharyngeal
carcinoma when compared with PET-CT
– [Comoretto M,et al]
2/25/2018 26](https://image.slidesharecdn.com/headandneckreirradiation-180225024531/85/Head-and-neck-reirradiation-26-320.jpg)
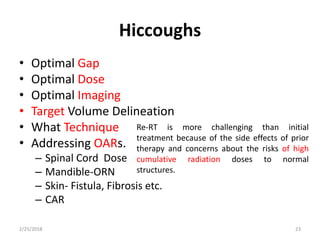
![Addressing OARs.
• Vital
– Cord
– Optic apparatus
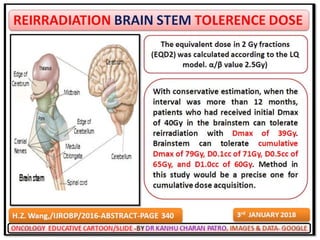
– Brain[temporal lobe, Brain stem]
• Less vital
– Cochlea
– Carotid
– Parotid
– mandible
2/25/2018 46
keep in mind ,The α/β of
prior irradiated tissue is not
the same as
Non-irradiated tissue](https://image.slidesharecdn.com/headandneckreirradiation-180225024531/85/Head-and-neck-reirradiation-46-320.jpg)
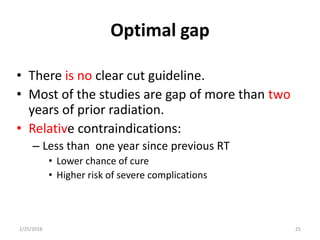
![Complication-acute toxicity
• MUCOSITIS
– The rate of grade 3–4 mucositis was lower for previously
irradiated patients. More contemporary trials have
demonstrated similar results.
– Primary CRT is associated with higher rates of grade 3–4
mucositis (71–77%) when compared with CRRT (14–26%). This is
probably due to the smaller RT target volumes that are
commonly used for a course of salvage Re-RT
• [Brizel DM et al, Calais G et al]
• HEMATOLOGIC TOXICITY
– Hematologic toxicity appears to correlate with the intensity of
the systemic therapy regimen and is also not influenced by prior
therapy
• DEATH DURING TREATMENT
– This may be related to the fact that functional reserve is
compromised in heavily pretreated patients[Glisson BS et al]
2/25/2018 47](https://image.slidesharecdn.com/headandneckreirradiation-180225024531/85/Head-and-neck-reirradiation-47-320.jpg)
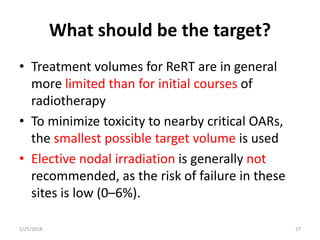
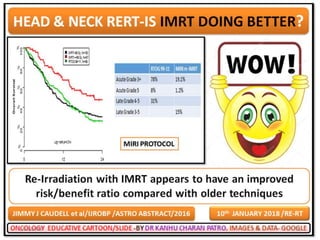
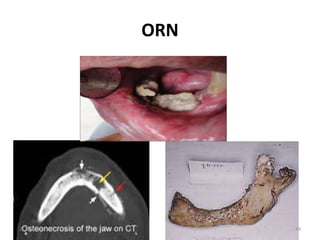
![Complication-Late toxicity-ORN
• It is possible that the rates of ORN are less in patients
treated with more modern radiotherapy techniques for
CRRT. Increasing photon energies, 3DCRT and IMRT
ameliorate this phenomenon.
• One series, cases of ORN only occurred in patients
receiving a cumulative RT dose of greater than 120 Gy
– [De Crevoisier R et al, Sulman EP et al]
• In a cohort of 105 patients treated between 1996 and
2005, 70% of whom received IMRT, only one case of grade
2 osteitis was reported.
– [Lee N et al]
• In another cohort of 74 patients all treated with IMRT
between 1999 and 2004, only 5% developed ORN
– [Sulman EP et al]
2/25/2018 48](https://image.slidesharecdn.com/headandneckreirradiation-180225024531/85/Head-and-neck-reirradiation-48-320.jpg)
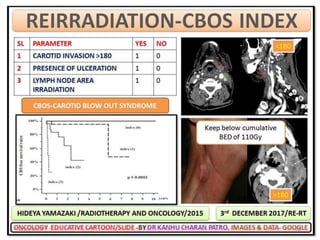
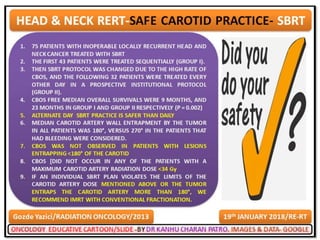
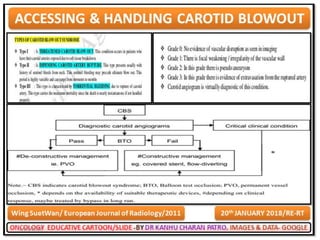
![Carotid artery rupture (CAR)
• Devastating condition due to
– Tumor recurrence,
– Chronic infection,
– Surgery (pharyngocutaneous fistula and neck dissection),
– Poor nutrition
– Chronic inflammation
– (long-term tracheostomy and nasogastric tubes)
A meta-analysis of CRRT trials reporting CAR showed a
crude incidence rate of 2.6% at a median of 7.5 months
following CRRT
[McDonald MW et al]
2/25/2018 60](https://image.slidesharecdn.com/headandneckreirradiation-180225024531/85/Head-and-neck-reirradiation-60-320.jpg)
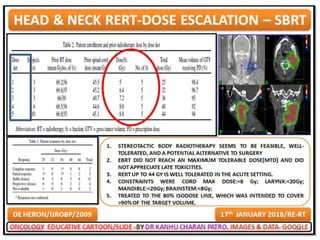
![TPZ STUDY
• 25 patients received cisplatin (50 mg/m2) and TPZ (260
mg/m2) on weeks 1, 3 and 5 during daily RRT to a total
dose of 72 Gy.
• Additional TPZ (160 mg/m2) was given on days 1, 3 and
5 of week 2, and possibly week 4, based on
randomization.
• Locoregional control was 56% overall and the 1- and 2-
year rates of OS were 56 and 27%, respectively.
• Treatment-related toxicity was comparable with other
CRRT trials
– Dische S. Chemical sensitizers for hypoxic cells: a decade
of experience in clinical radiotherapy. Radiother.
Oncol.3(2), 97–115 (1985)]
2/25/2018 69](https://image.slidesharecdn.com/headandneckreirradiation-180225024531/85/Head-and-neck-reirradiation-69-320.jpg)
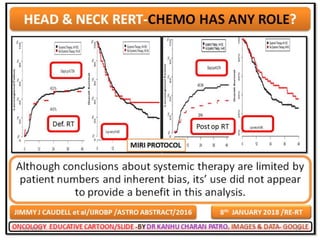
![Role of chemotherapy
• Still to be established.
• NACT
– for high volume disease
– Prolonging the period for Re-RT
• CONC.
• Mostly as radio-sensitizer
• Common drugs
– HFX REGIMEN-[HU+5FU+RT]
– Cisplatin
– Carboplatin
– Taxanes
– Gemcitabine
– Cetuximab/Biomab
2/25/2018 70](https://image.slidesharecdn.com/headandneckreirradiation-180225024531/85/Head-and-neck-reirradiation-70-320.jpg)
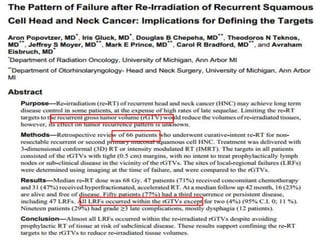

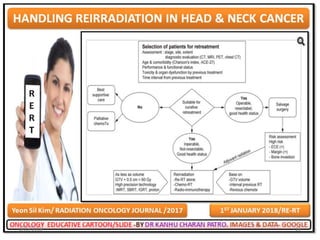
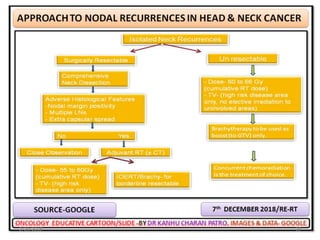
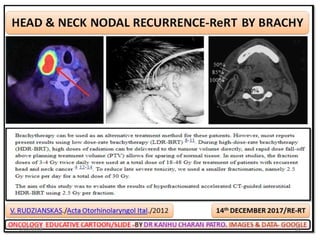
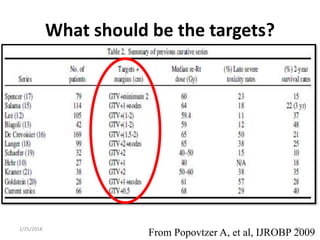
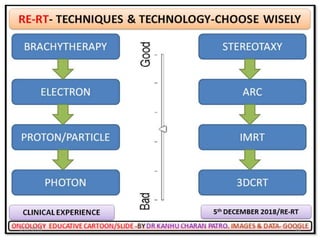
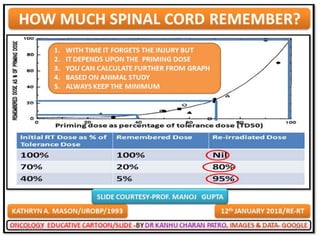
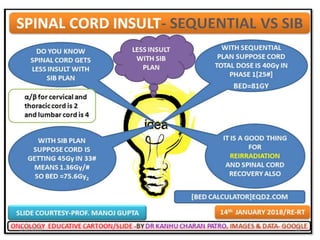
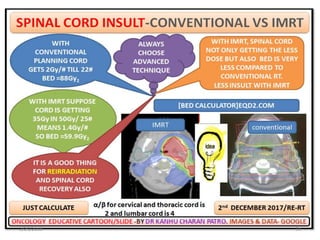
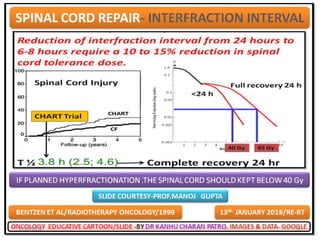
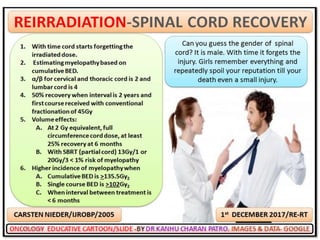
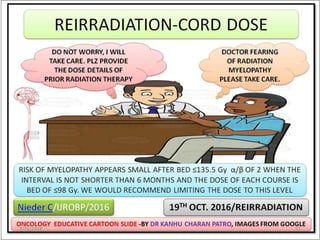
This document discusses reirradiation in recurrent head and neck cancer. It notes that radiation therapy plays a central role in head and neck cancer treatment but recurrence still occurs in 20-35% of patients. Reirradiation presents challenges due to prior radiation exposure and damage to normal tissues. The document discusses treatment options, appropriate patient selection, techniques like IMRT to minimize dose to organs at risk, optimal timing and dosing of reirradiation, and management of toxicities.













































































![Hypothalamus short ppt by Dr. Neha [PT].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/hypothalamusbydr-260124145759-b9f94a93-thumbnail.jpg?width=640&height=640&fit=bounds)









