Downloaded 1,001 times



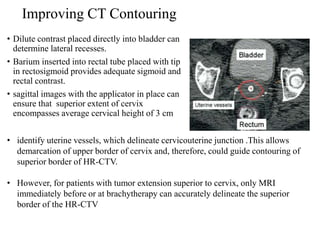

The document discusses advances in brachytherapy for cervical cancer, including new applicator developments, imaging modalities, and treatment planning systems. It outlines the American Brachytherapy Society's recommendations for image-guided brachytherapy (IGBT) and highlights the criteria for patient selection and treatment protocols. Additionally, it emphasizes the importance of volumetric imaging and advanced dosimetry in achieving optimal treatment outcomes while addressing the limitations of traditional imaging methods.










































![Management Of Early Stage Ca Cervix [Autosaved]](https://cdn.slidesharecdn.com/ss_thumbnails/management-of-early-stage-ca-cervix-autosaved-1233338415127954-2-thumbnail.jpg?width=640&height=640&fit=bounds)
































































