Downloaded 209 times
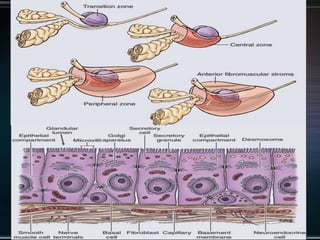
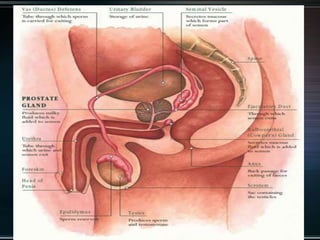
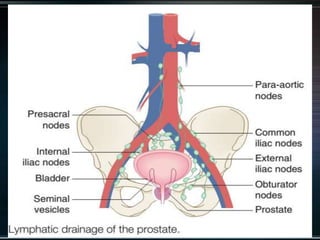
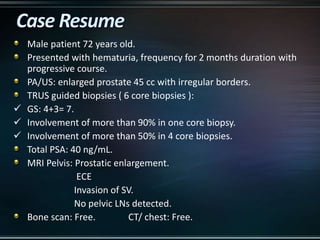
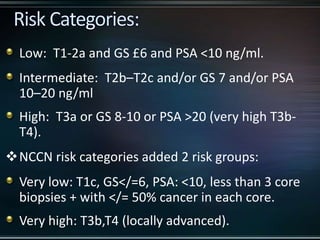
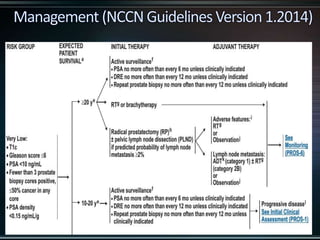
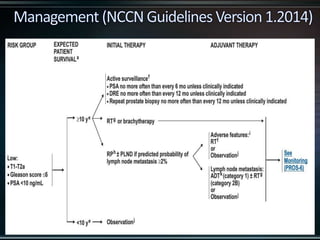
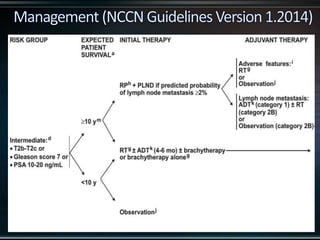
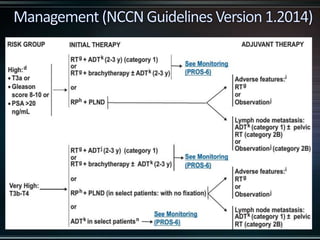











This document discusses prostate cancer and its treatment with radiation therapy. It provides details on: 1) The anatomy of the prostate gland and the cell types that compose normal prostate epithelium. 2) A case presentation of a 72-year-old male with high-risk prostate cancer. 3) Guidelines for risk stratification and treatment recommendations including neoadjuvant androgen deprivation therapy followed by radiation therapy with concurrent and adjuvant androgen deprivation therapy.























































































