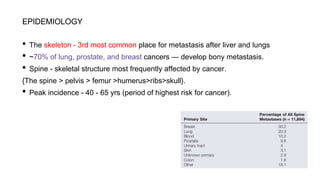
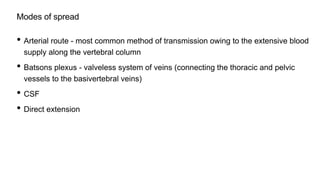
This document summarizes key points about spinal metastasis including epidemiology, symptoms, diagnostic imaging, and treatment approaches. Spinal metastasis most commonly affects the thoracic spine and presents as back pain in 70-95% of patients. Imaging plays an important role in diagnosis, with MRI and CT being most sensitive and specific. Treatment depends on factors such as neurological involvement, tumor type, and mechanical stability, and may include radiation, surgery, chemotherapy, or bisphosphonates. The goal of treatment is pain relief and preservation of neurological function.























































![제 23회 보아즈(BOAZ) 빅데이터 컨퍼런스 - [MBOAX] : ABSA를 활용한 소비자 반응 분석 기반 운영 효율화 대시보드 설계](https://cdn.slidesharecdn.com/ss_thumbnails/3-1boaz23rdconferencemboax-260203102709-9d519923-thumbnail.jpg?width=640&height=640&fit=bounds)

















![7.__Developing_a_Research_Proposal[1].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/7-260131073037-df92dd7d-thumbnail.jpg?width=640&height=640&fit=bounds)