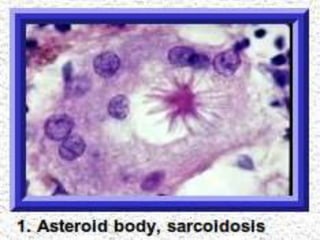
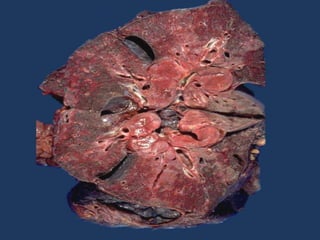
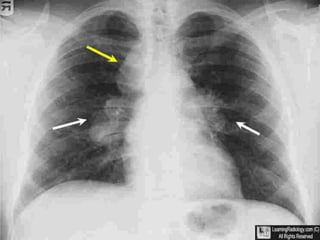
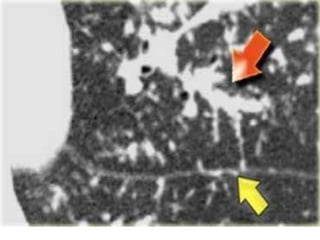
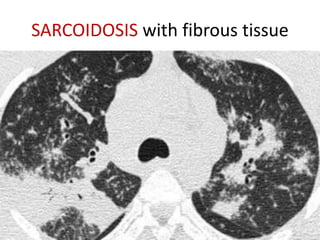
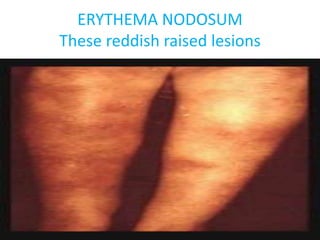
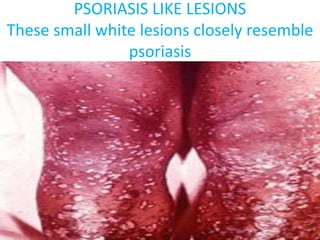
Sarcoidosis is a multisystem granulomatous disorder of unknown etiology characterized by non-caseating granulomas. It most commonly affects the lungs presenting as bilateral hilar lymphadenopathy and pulmonary infiltrates. Extrapulmonary involvement can include the skin, eyes, liver and musculoskeletal system. Diagnosis involves clinical features and exclusion of other causes. Treatment involves corticosteroids while prognosis depends on organ involvement with lung fibrosis carrying the worst prognosis.