Downloaded 146 times


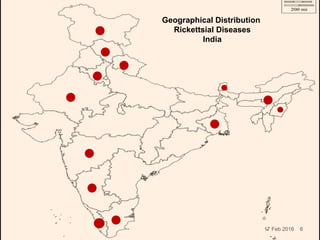
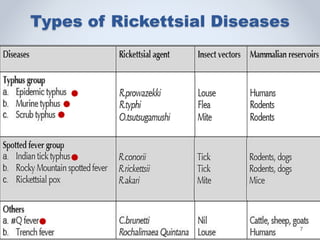
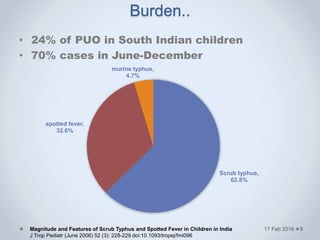
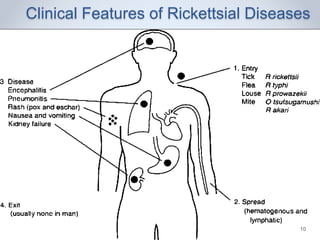
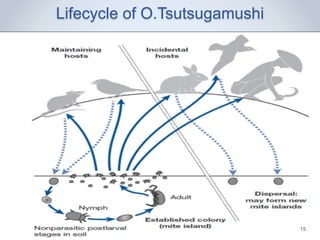
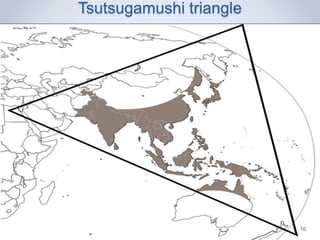
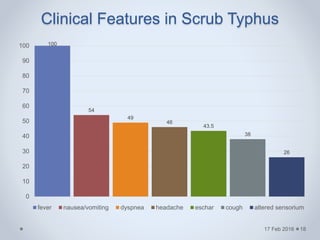
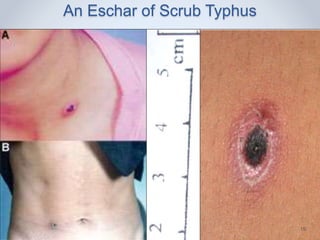
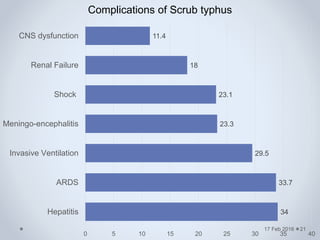
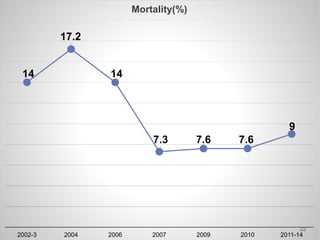

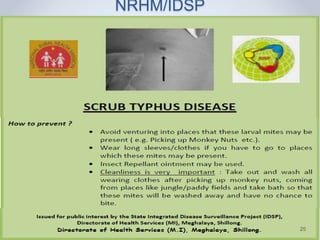

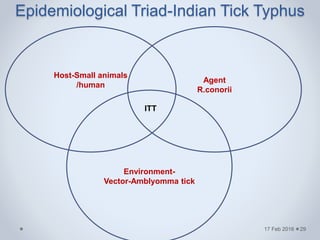
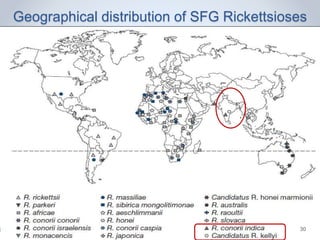
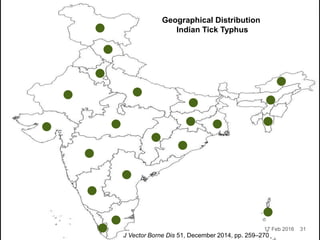

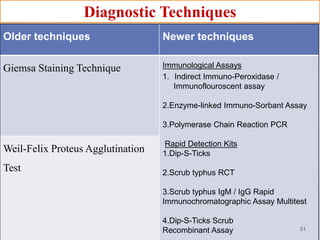
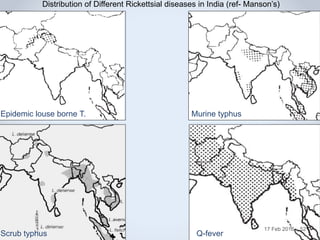


This document summarizes rickettsial diseases in India, including scrub typhus, Indian tick typhus, murine typhus, Q fever, and epidemic louse-borne typhus. It discusses the epidemiology, clinical features, diagnosis, treatment, and prevention of these diseases. It notes that rickettsial diseases are re-emerging in India and can cause significant morbidity and mortality if not diagnosed and treated in a timely manner. The presentation provides details on the distribution, transmission cycles, symptoms, and outbreaks of each disease in India.































![RIKETTSIAL DISEASE IN INDIA [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/rikettsialdiseaseautosaved-240331142139-5d5a8fb7-thumbnail.jpg?width=640&height=640&fit=bounds)














































![Hypothalamus short ppt by Dr. Neha [PT].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/hypothalamusbydr-260124145759-b9f94a93-thumbnail.jpg?width=640&height=640&fit=bounds)








