Laser retinal therapy uses lasers to treat various retinal conditions:
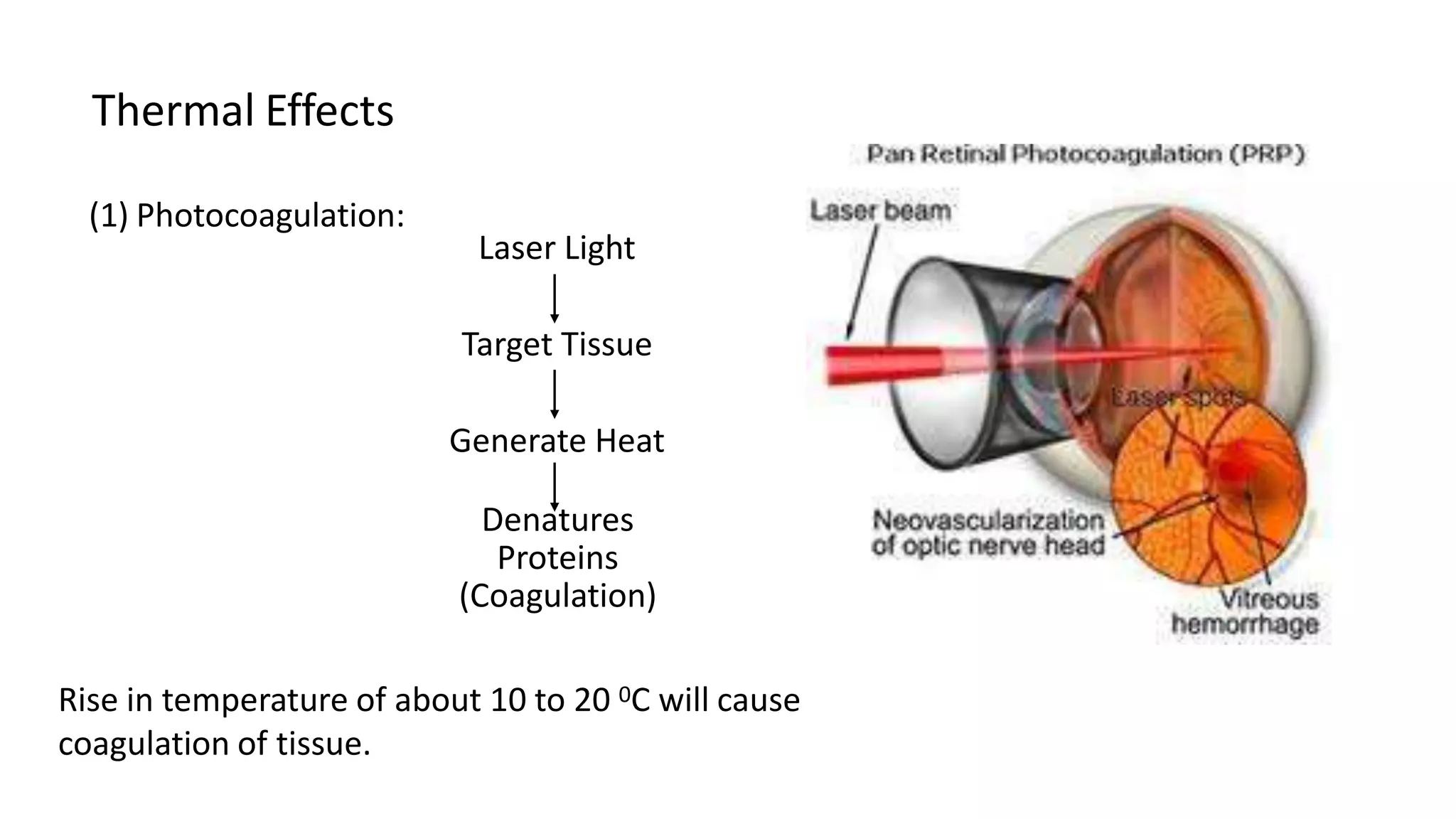
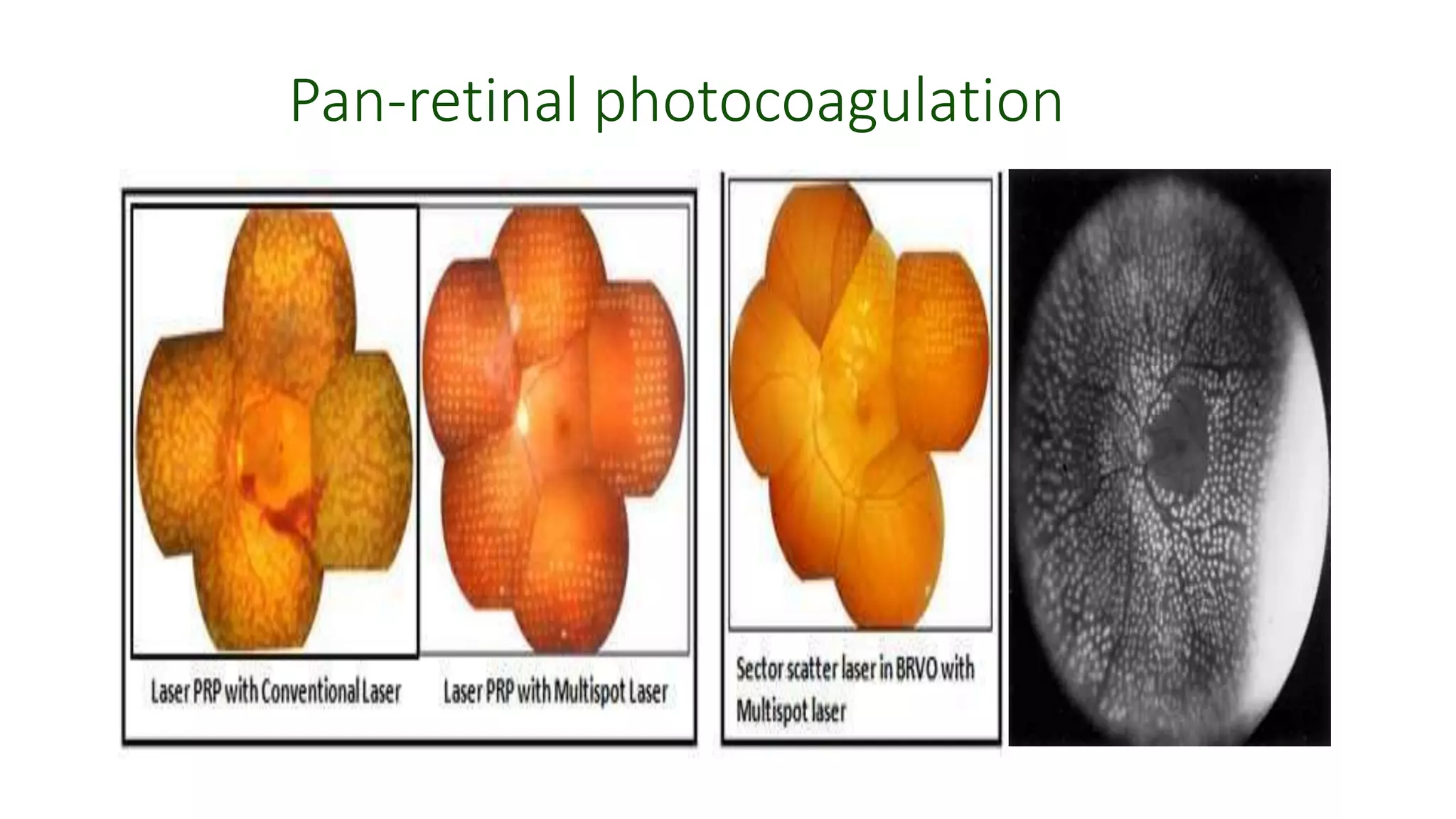
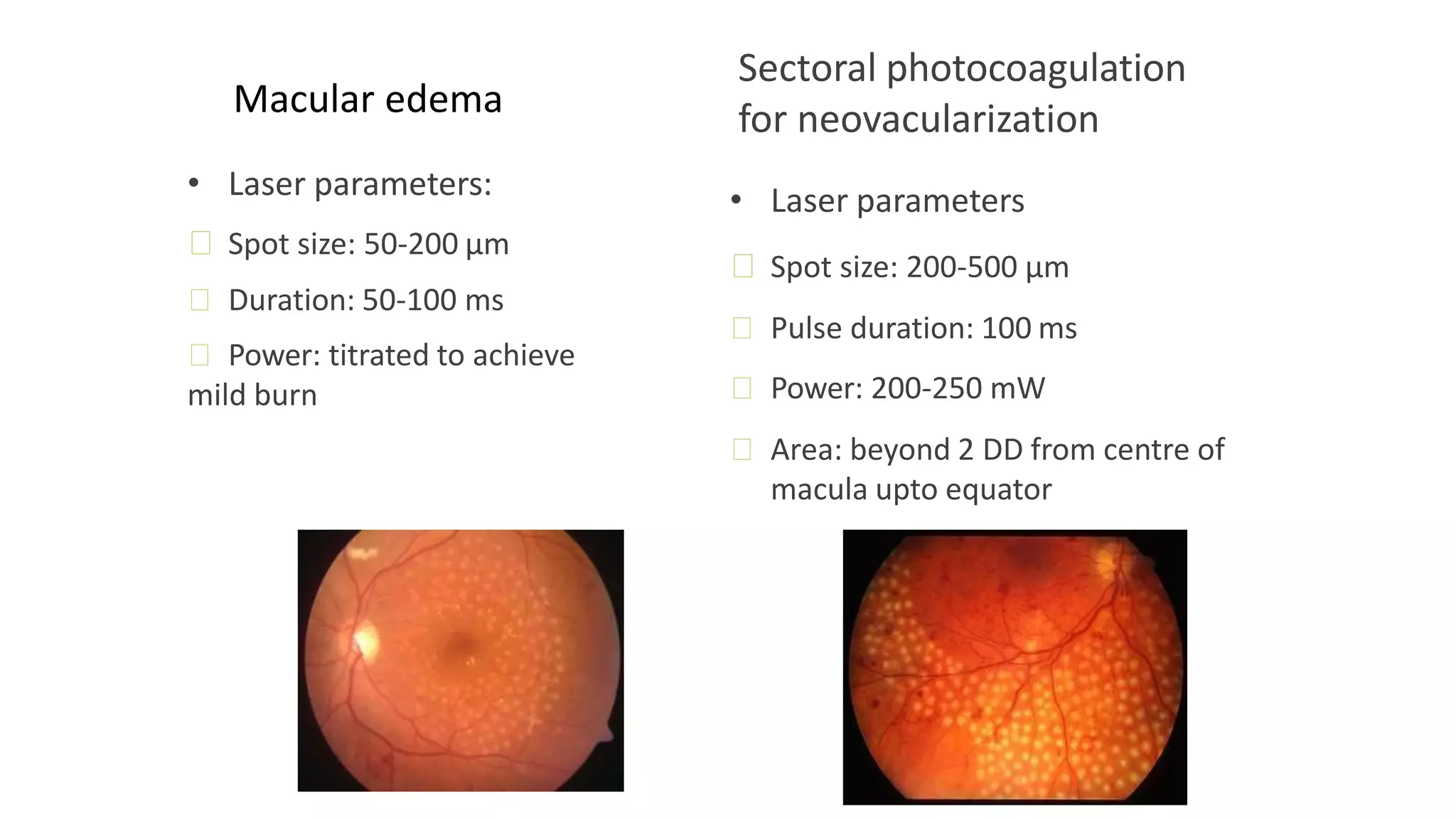
1. Pan-retinal photocoagulation uses lasers like argon to treat diabetic retinopathy by reducing retinal ischemia.
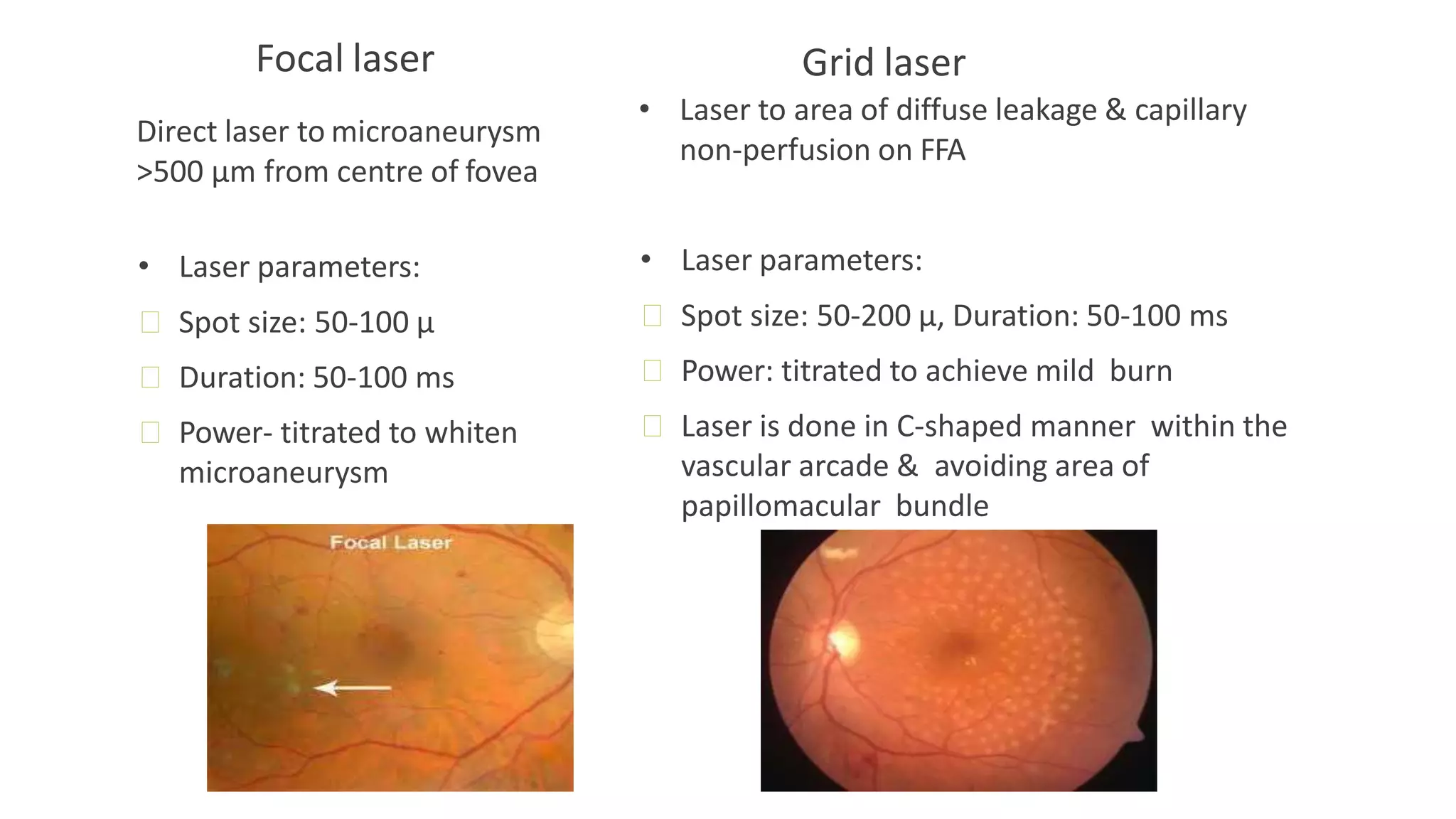
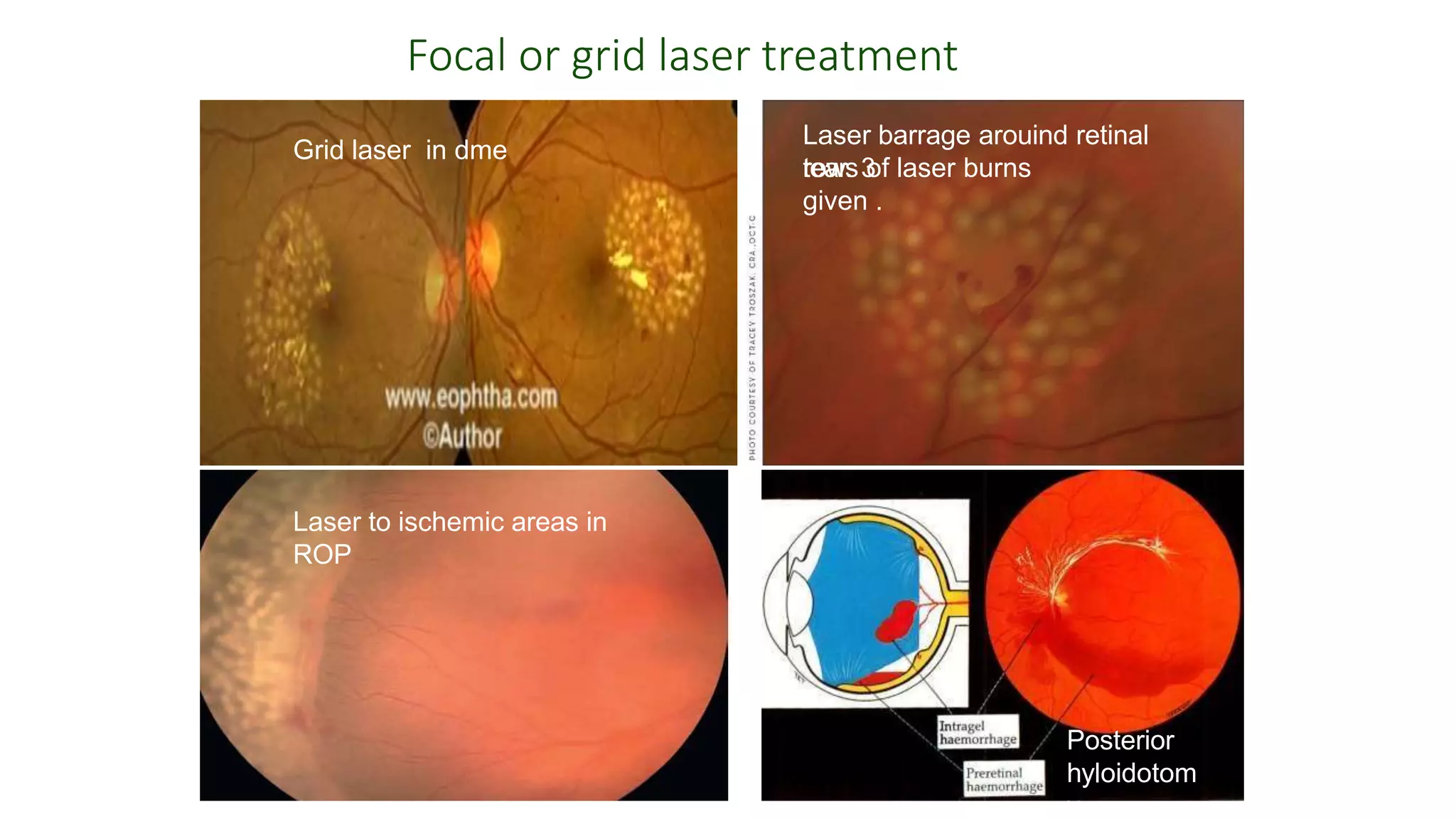
2. Macular edema is treated with focal or grid laser photocoagulation targeted at leaking microaneurysms or diffuse areas of leakage.
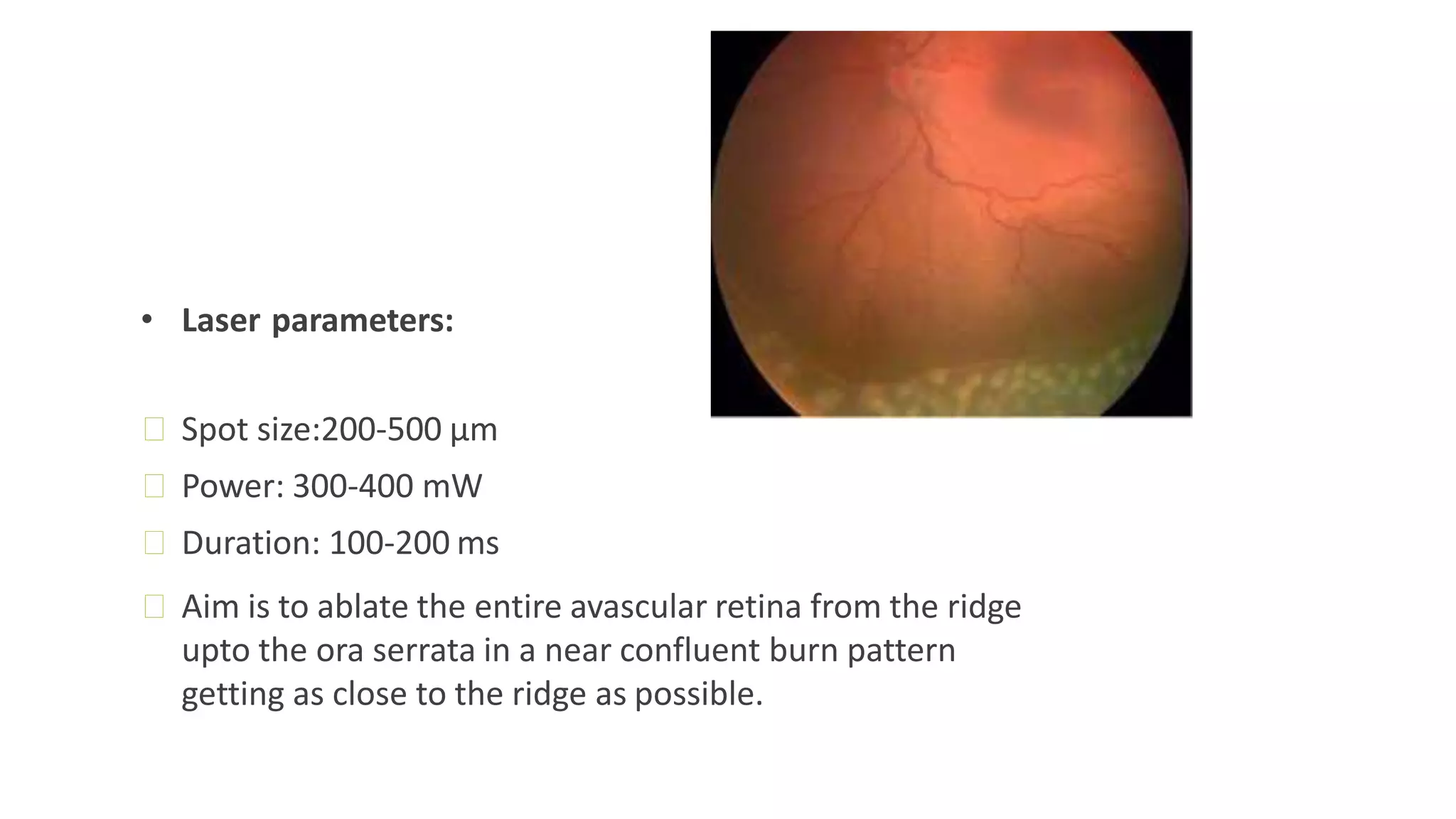
3. Retinal tears and detachments are treated preventatively with laser barrage surrounding tears to stimulate proliferation and adhesion.