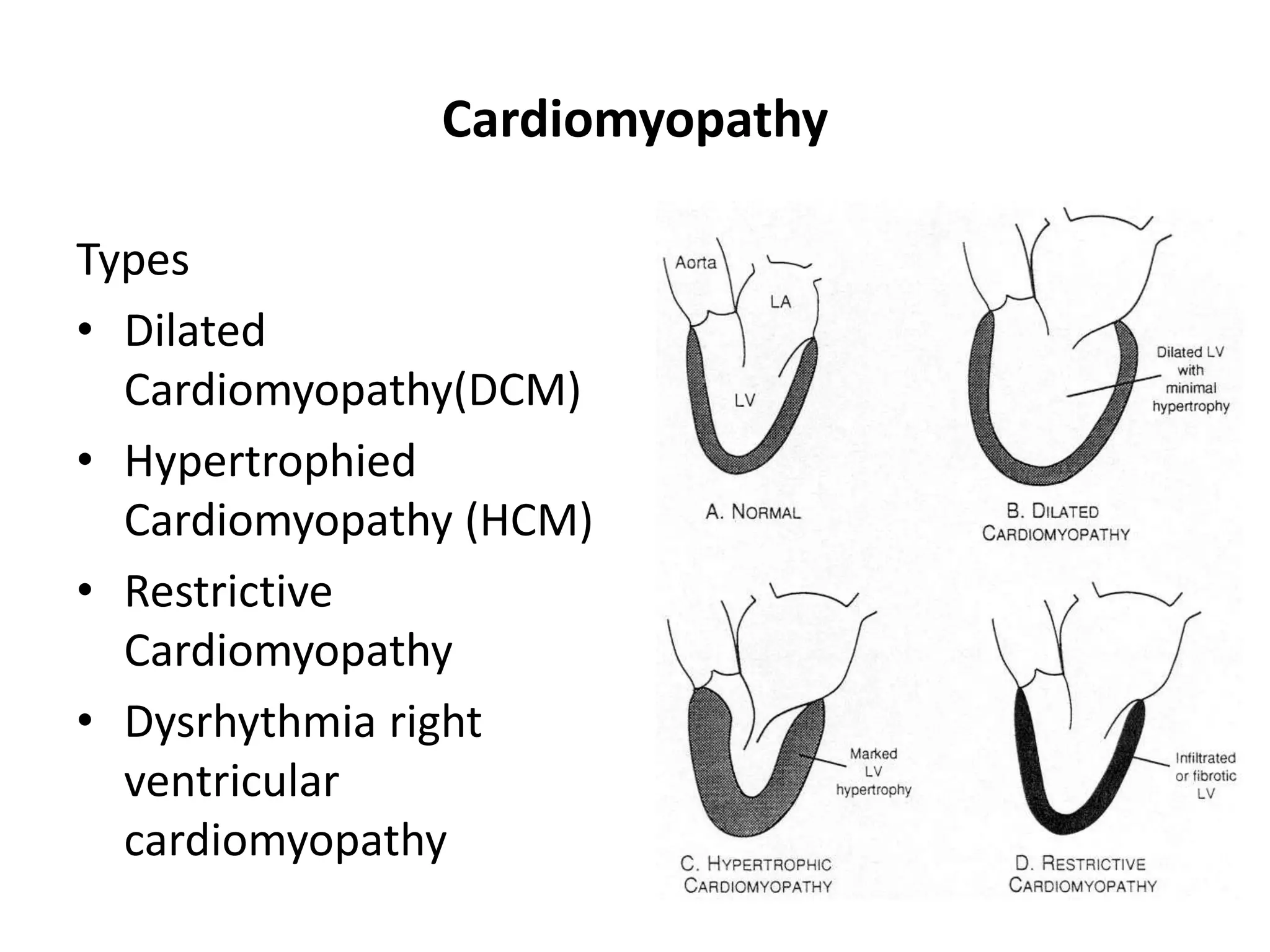
The document provides an overview of cardiomyopathy, myocarditis, and pericardial diseases for nursing students. It defines cardiomyopathy as a heterogeneous group of diseases affecting the heart muscle and lists the main types as dilated, hypertrophic, and restrictive cardiomyopathy. Myocarditis is defined as inflammation of the heart muscle and pericarditis as inflammation of the pericardium. The document describes the causes, clinical presentations, diagnoses, and treatments of these conditions.
























![Management_HCM
• Enhance impaired LV diastolic function(improve filling)
Slow heart rate
Maintain normal sinus rhythm[Drugs to enhance
myocardial relaxation]
• Reduce obstruction caused by septal/MV apposition:
Avoid dehydration and vasodilators
Negative inotropic drugs (beta blockers, disopyramide)
Surgical septal myectomy
Dual chamber (atrial and ventricular) pacemaker](https://image.slidesharecdn.com/cardiomyopathymyocarditisandpericarditiscilectureoct-231003122417-bc0aefcc/75/Cardiomyopathy-Myocarditis-and-Pericarditis_C-I-lecture_Oct-ppt-27-2048.jpg)



































































































































