Downloaded 165 times























































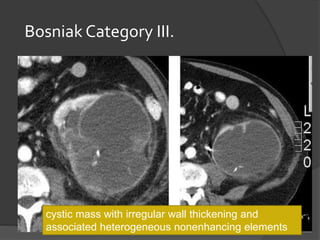




















This document describes a case of a 48-year-old male patient presenting with right lumbar pain and swelling for 9 months and 3 months respectively. On examination, a non-tender cystic mass was palpable in the right lumbar region. Investigations including ultrasound and CT scan revealed a renal cyst. The document then provides an overview of renal cysts, discussing simple cysts, complicated cysts, and the Bosniak classification system for cystic renal masses. Based on imaging findings, the patient's cyst was likely a Bosniak Category II cyst.











































































































