Downloaded 153 times

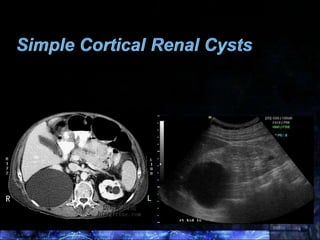





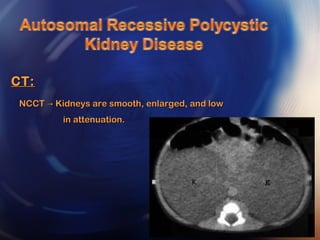
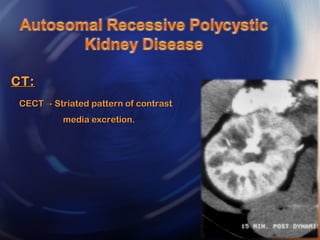

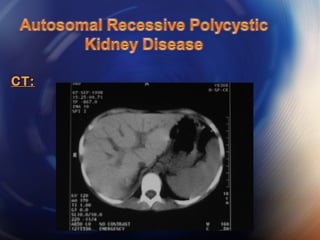


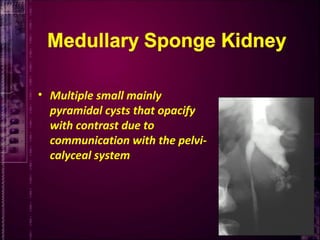
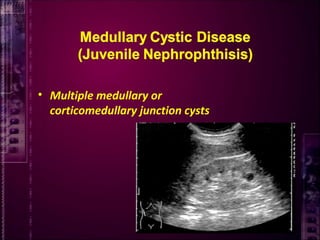


This document discusses various renal cystic diseases and conditions. It covers cortical and medullary cysts, polycystic kidney disease, multicystic renal dysplasia and extra-parenchymal cysts. Autosomal dominant polycystic kidney disease is described as the most common hereditary cystic renal disease affecting 1 in 1000 people typically in the third decade of life. Imaging findings for simple cysts, polycystic kidney disease, multicystic renal dysplasia and extrarenal cysts on ultrasound, intravenous urography, CT and MRI are summarized.











































































































