Downloaded 36 times

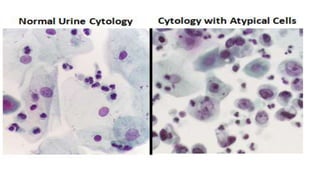





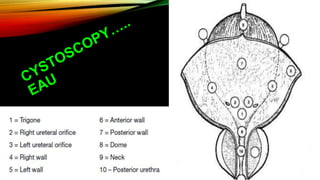
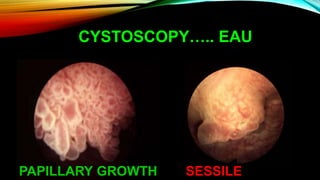
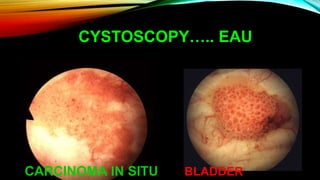


The document discusses various diagnostic modalities for urinary bladder carcinoma, highlighting the effectiveness and limitations of urine cytology, transabdominal ultrasound, computed tomography urography, and urinary molecular marker tests. Urine cytology is noted for its high sensitivity in detecting high-grade tumors but has limitations due to user dependency and false positives. Overall, while cystoscopy remains essential for diagnosis, molecular markers may assist in surveillance but cannot replace cystoscopy in routine practice.























































































