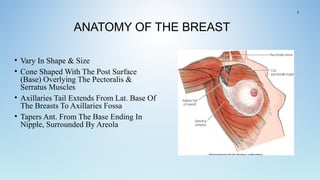
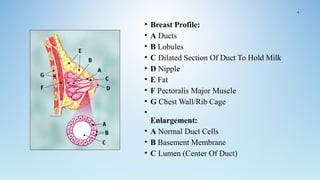
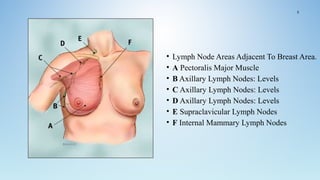
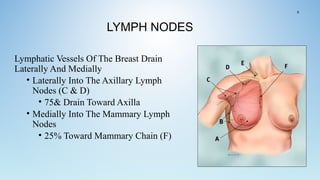
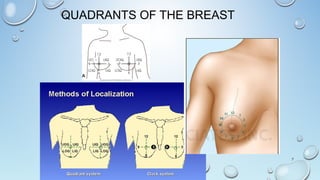
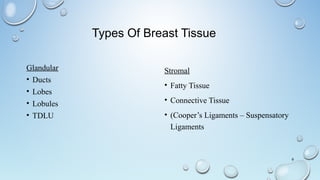
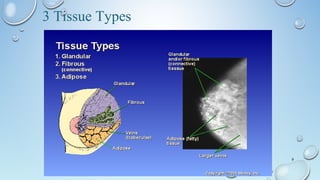
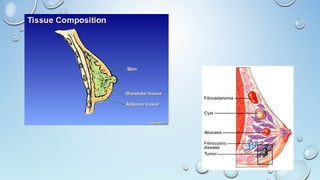
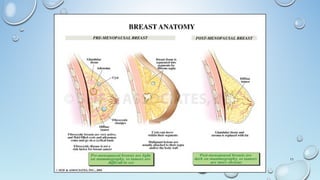
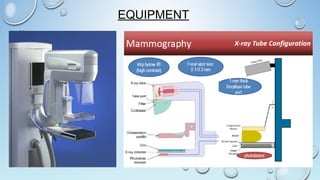
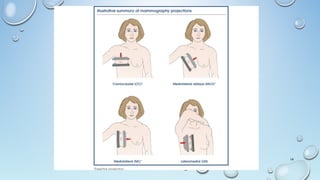
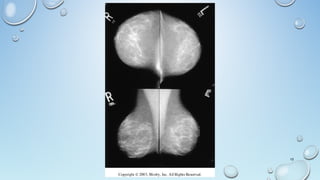
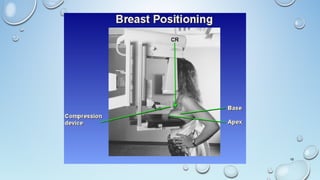
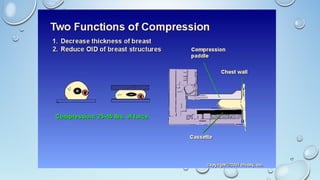
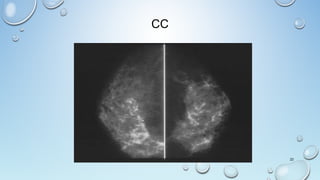
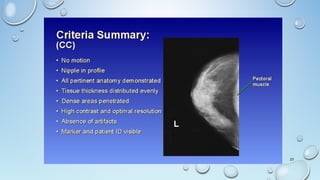
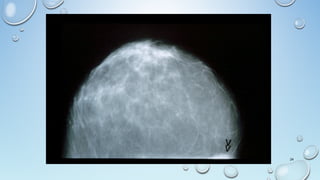
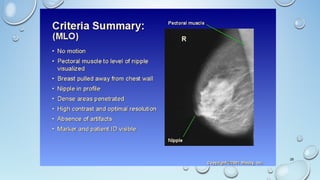
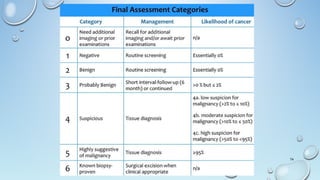
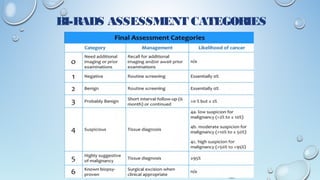
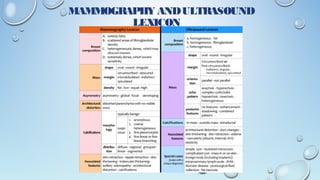
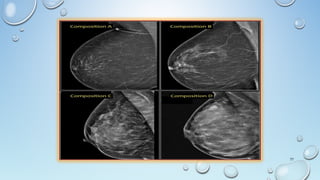
This document provides an overview of breast anatomy and mammography techniques. It describes the internal structures of the breast including lobes, lobules, ducts, and connective tissue. Lymph node drainage pathways are explained. Mammography views including craniocaudal, mediolateral oblique, and magnification views are illustrated along with positioning techniques. Breast composition changes with age. Ultrasound techniques and common breast lesions seen on ultrasound are also reviewed. The document concludes with an explanation of BI-RADS assessment categories used in breast imaging.







































































































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)



![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)





