Among the trials reviewed in 2016:
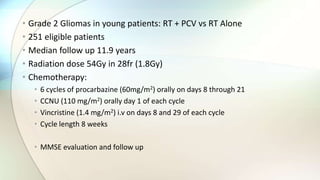
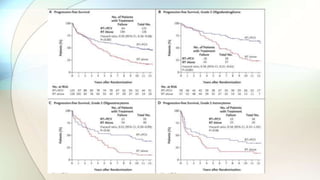
1) A study of grade 2 gliomas in young patients found that progression-free survival and overall survival were longer for those who received radiation therapy plus chemotherapy compared to radiation therapy alone.
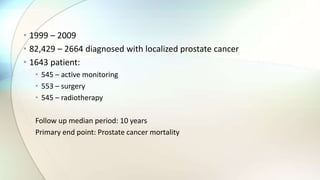
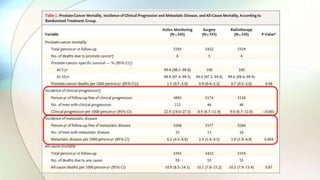
2) A prostate cancer study found that among men with localized prostate cancer, survival was similar for those undergoing surveillance with PET-CT scans compared to planned neck dissection, but surveillance resulted in fewer operations and was more cost-effective.
3) A soft-tissue sarcoma study found that overall survival was improved for patients receiving eribulin compared to an active control, suggesting eribulin could be a new treatment option for advanced soft-tissue sarcoma.
















































































![Hypothalamus short ppt by Dr. Neha [PT].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/hypothalamusbydr-260124145759-b9f94a93-thumbnail.jpg?width=640&height=640&fit=bounds)








