Downloaded 408 times

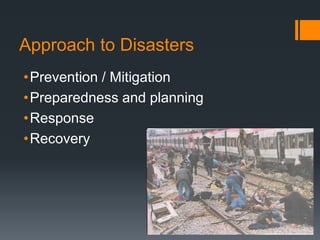
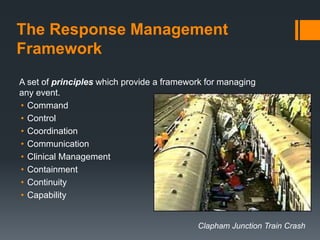


This document discusses principles of disaster management. It defines a disaster and outlines different types including natural and man-made disasters. Historical data shows disasters have increased over time and have significant economic and human costs. Disasters require a different approach than daily emergencies due to their scale and impact on infrastructure. The key principles of disaster management are prevention and mitigation, preparedness and planning, response, and recovery. An effective response follows a management framework of command, control, coordination, communication, and clinical management.





















































































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)

