Downloaded 233 times
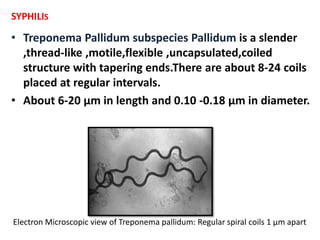
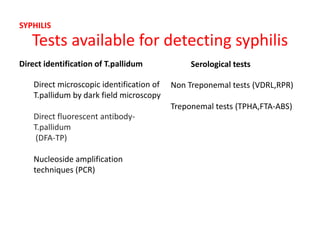
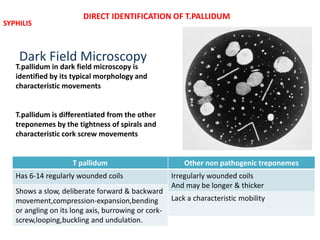
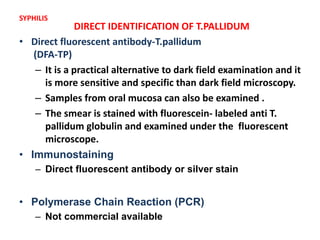
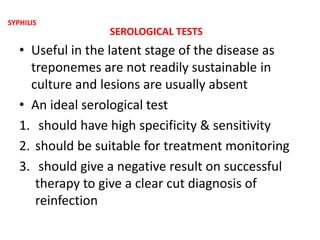
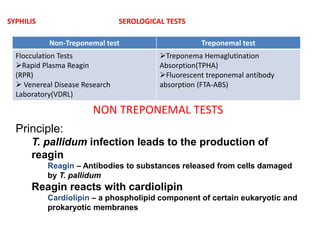
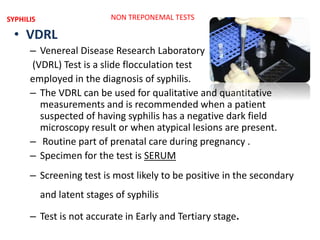

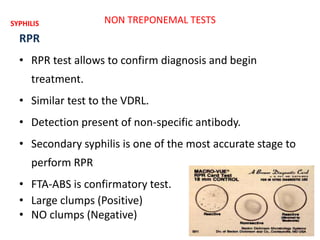
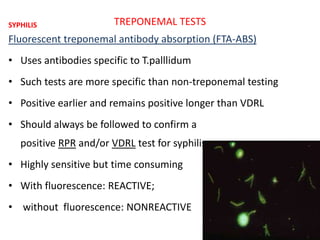

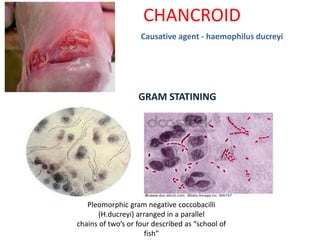
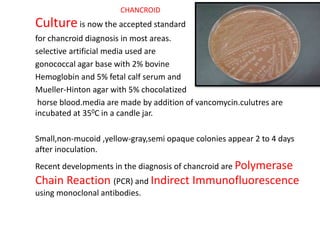

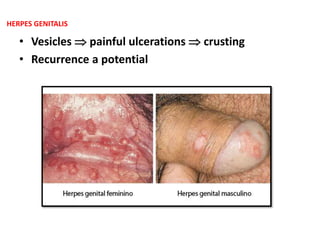
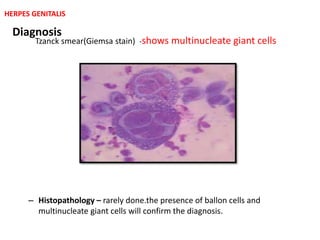
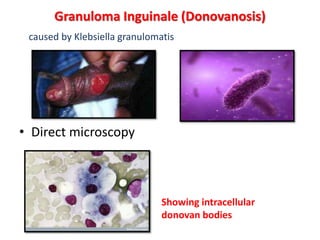
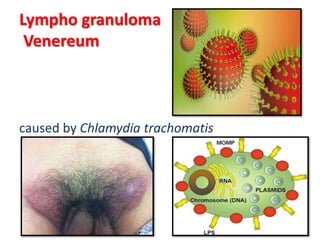









This document provides information on laboratory tests for diagnosing several common STIs/RTIs. It discusses the basic terminology used in laboratory testing and then focuses on specific organisms and the tests available to detect each one. For syphilis, it describes tests to directly identify Treponema pallidum such as darkfield microscopy as well as non-treponemal and treponemal serological tests. Similar information is provided on tests for gonorrhea, chlamydia, chancroid, herpes, donovanosis, lymphogranuloma venereum, and causes of genital discharge. Common laboratory techniques mentioned include microscopy, culture, PCR and various antigen or antibody detection methods.
















































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)


















![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)