Downloaded 35 times
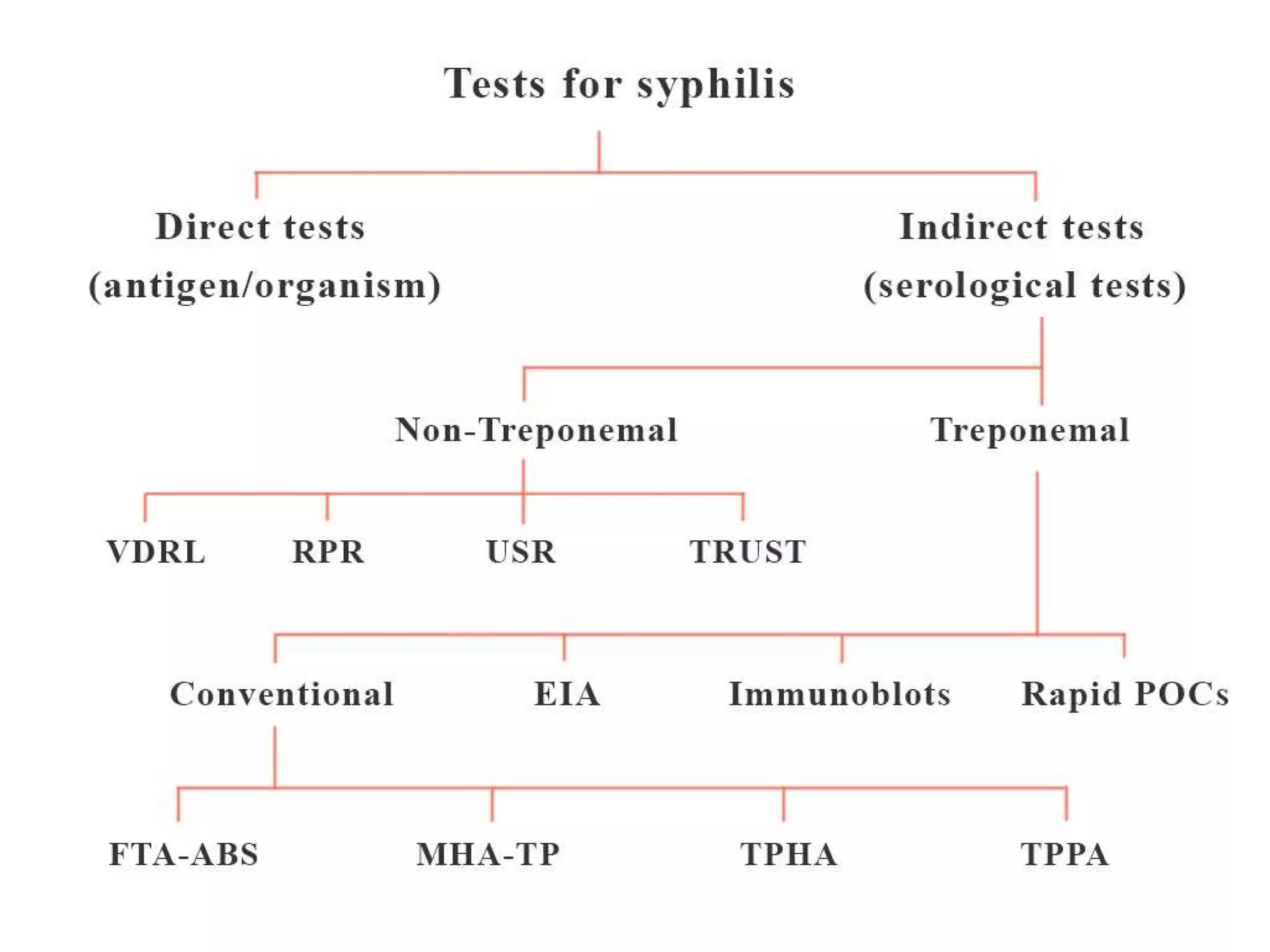
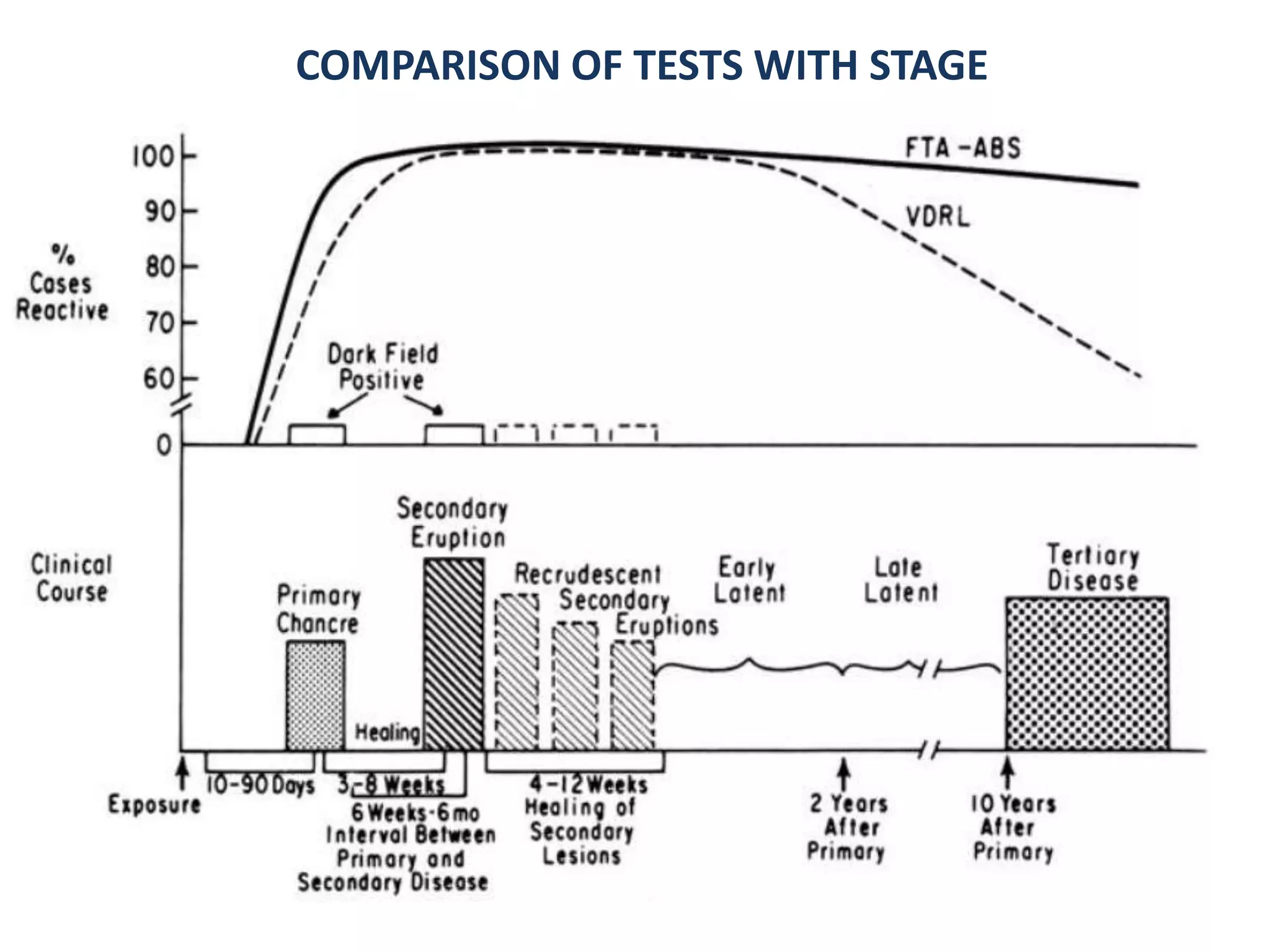
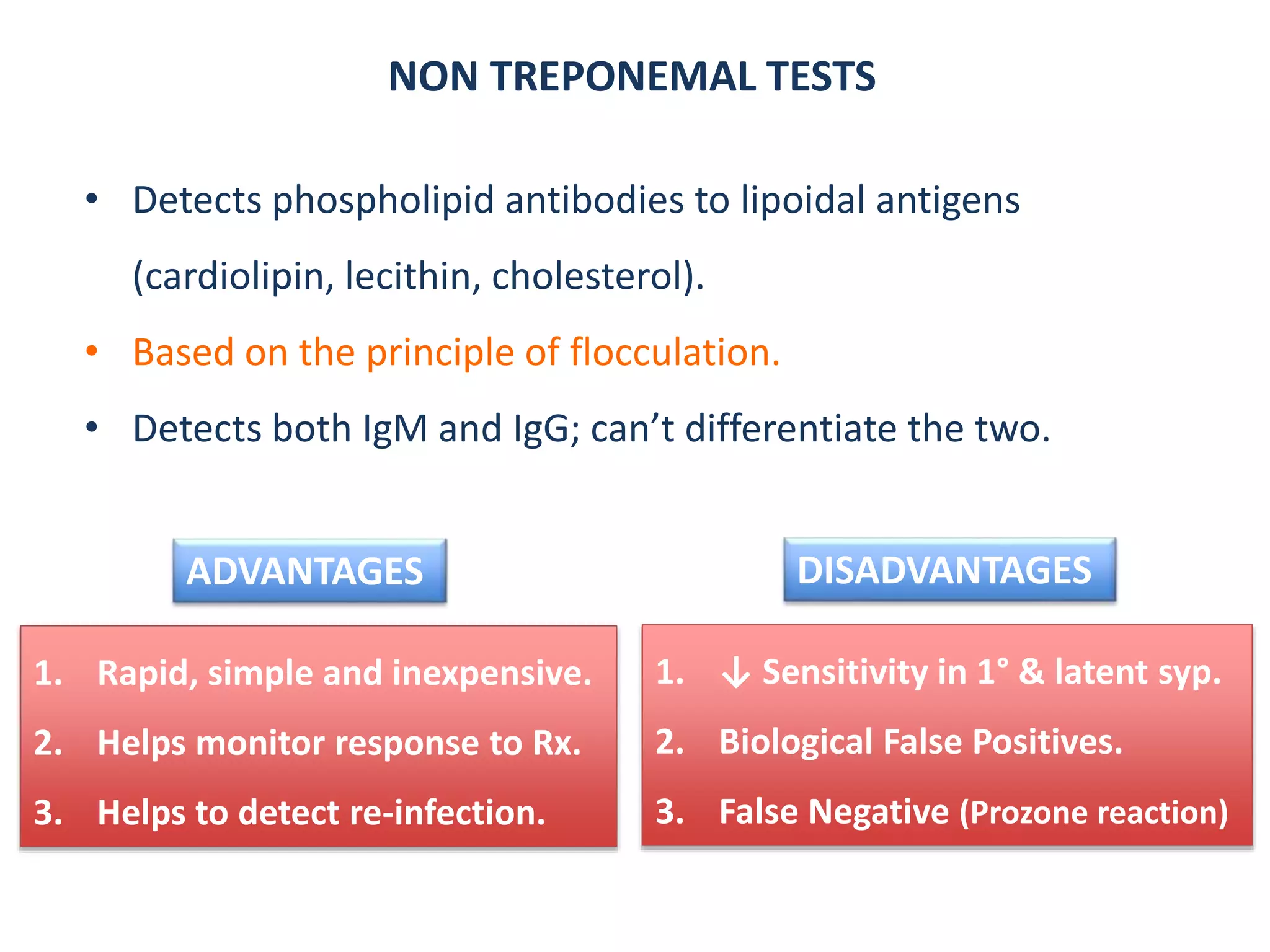
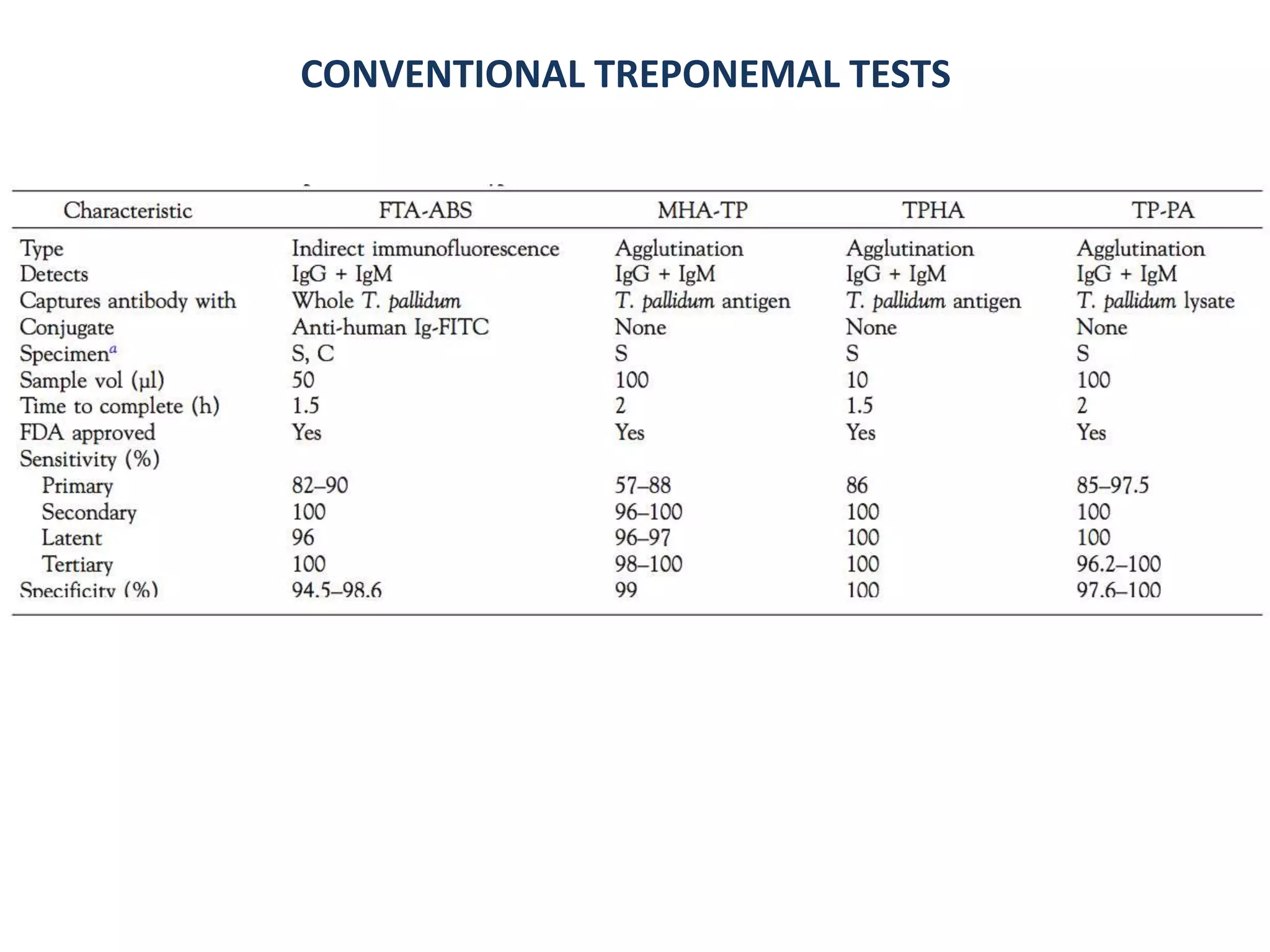
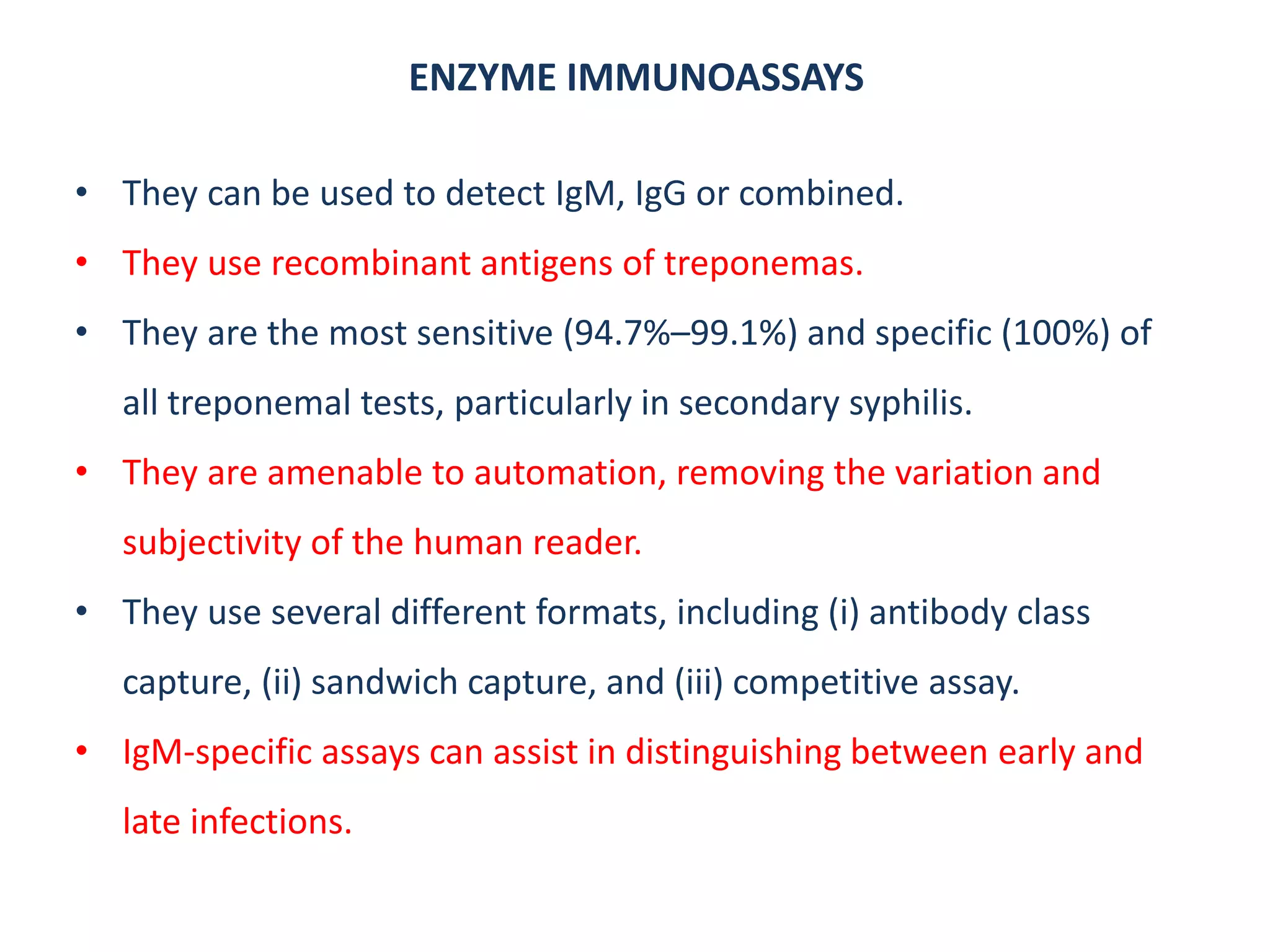
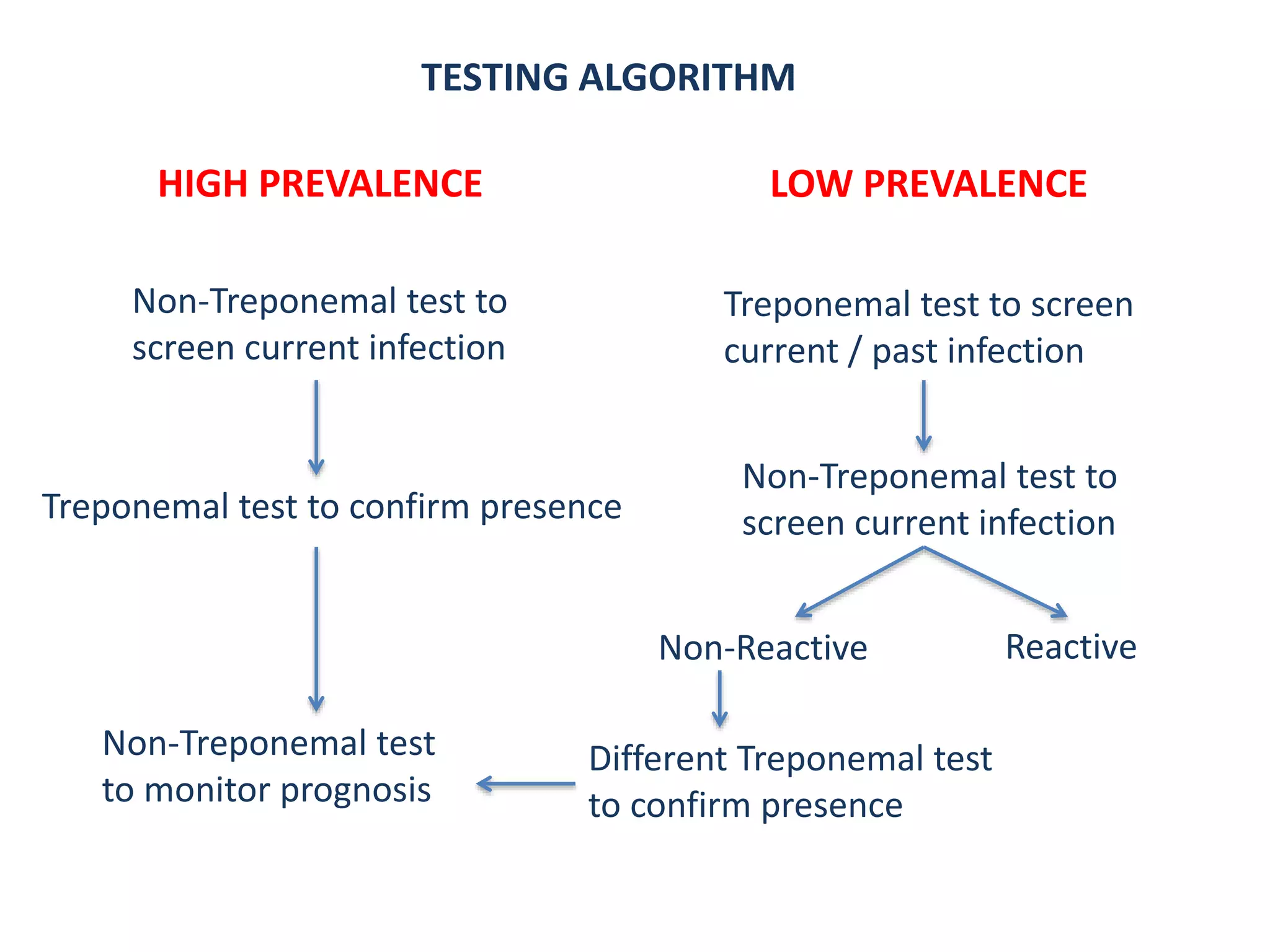
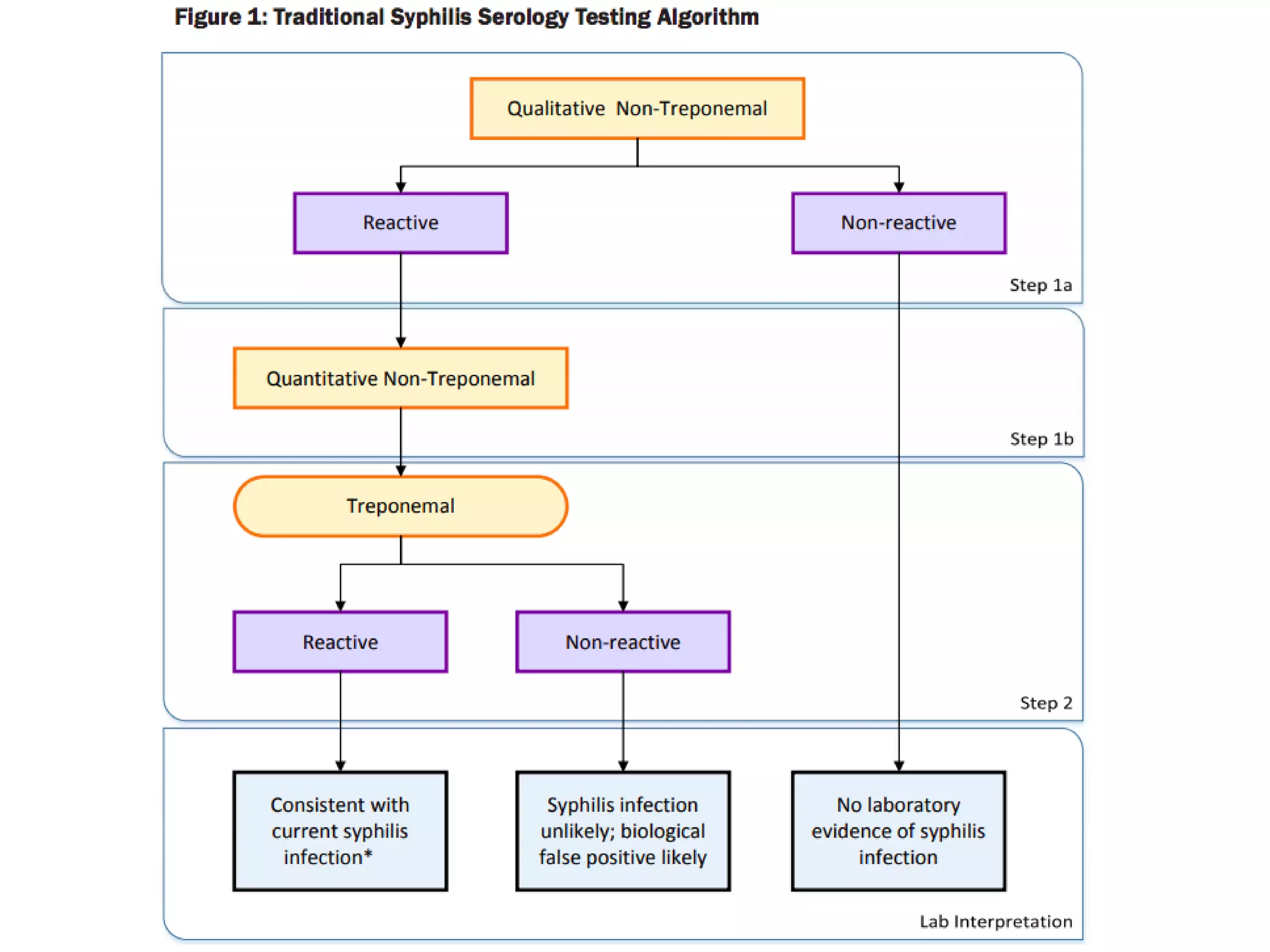
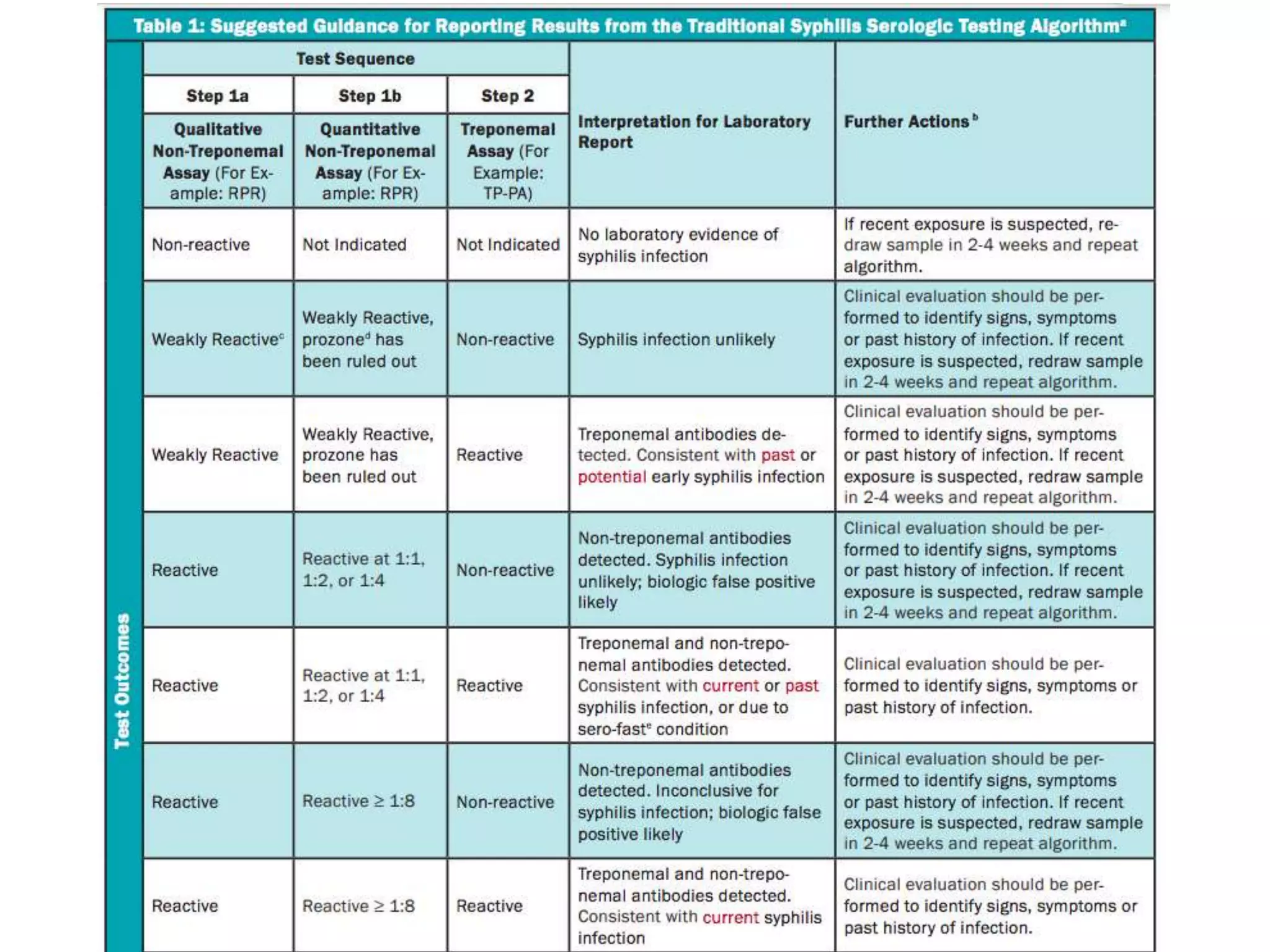
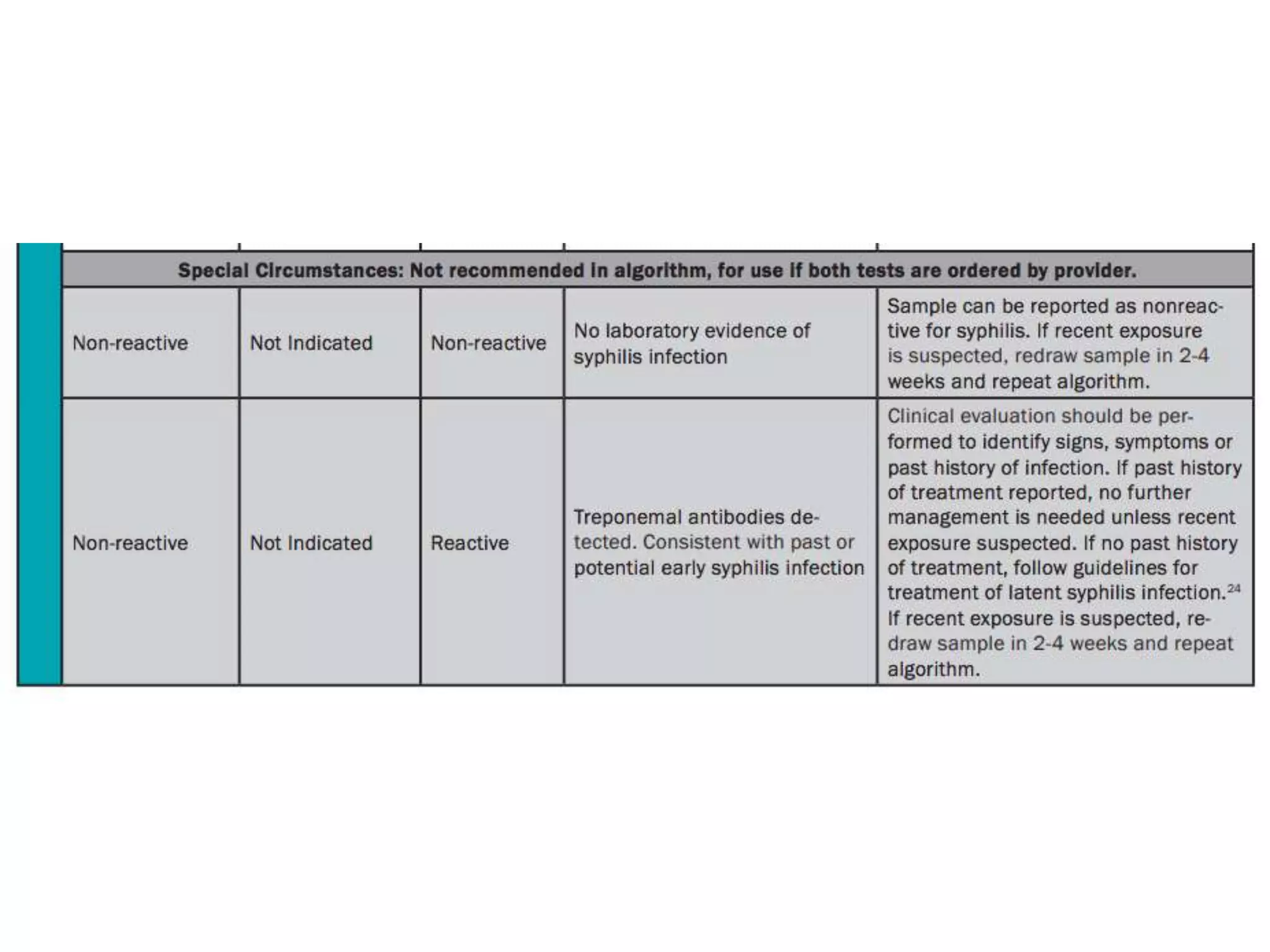
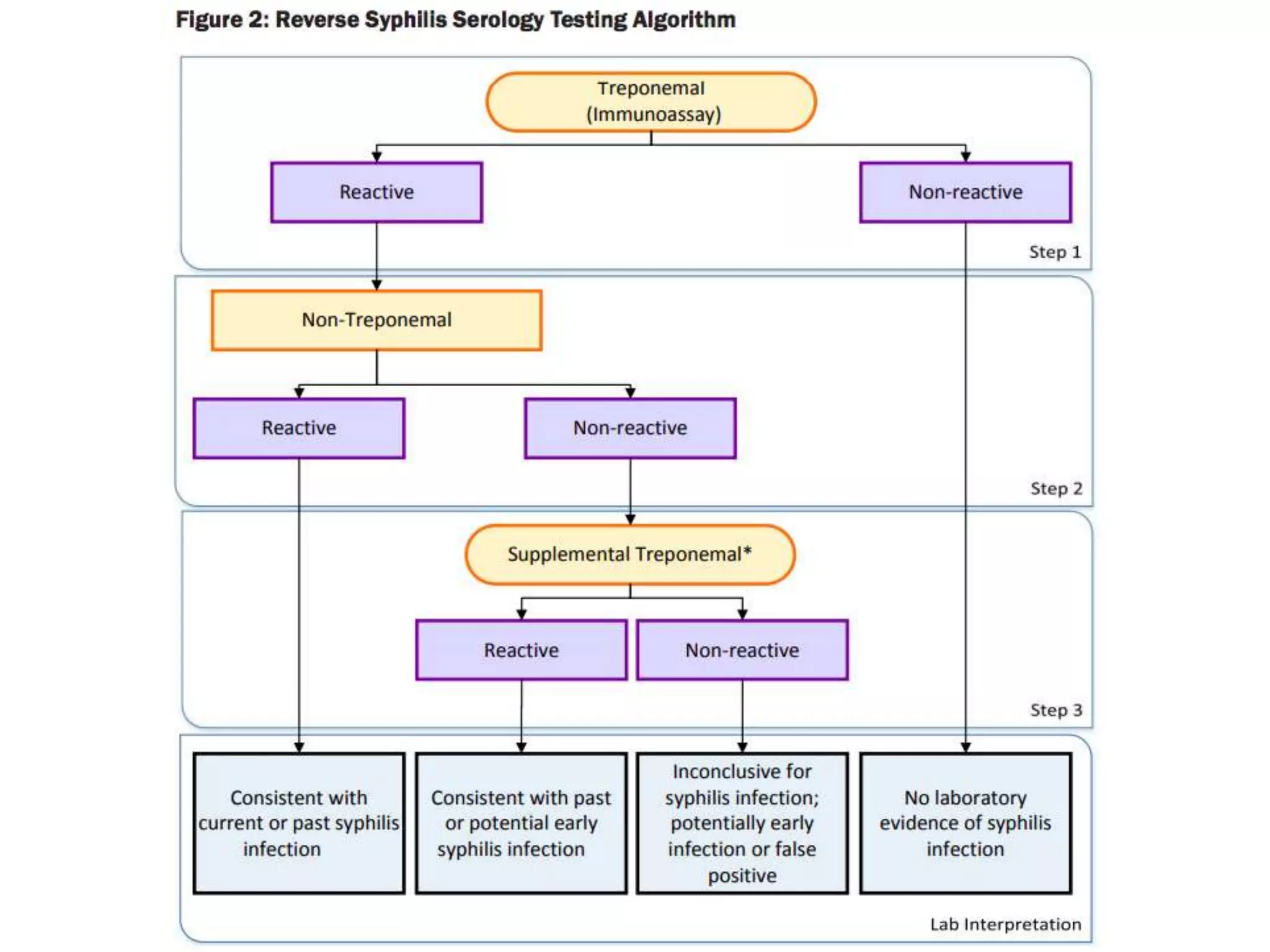

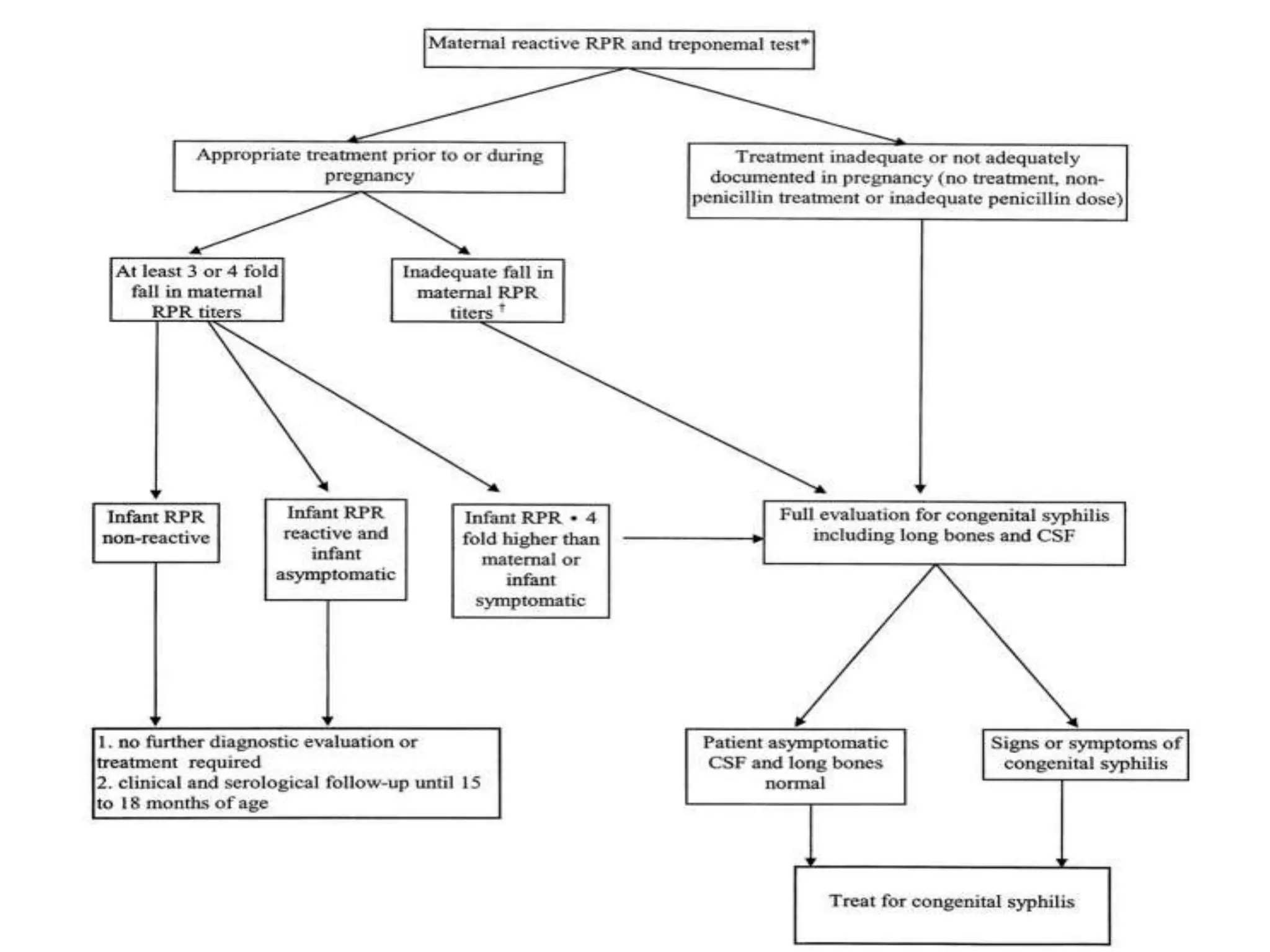

The document compares non-treponemal and treponemal tests for syphilis diagnosis, outlining their principles, sensitivities, and specificities. It emphasizes the advantages and disadvantages of each test type, recommending non-treponemal tests for screening and treponemal tests for confirmation of infection. Additionally, it discusses testing algorithms for congenital syphilis evaluation based on maternal serology results.






















































































