Downloaded 34 times
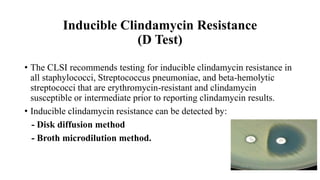


The document discusses the inducible clindamycin resistance test (D test) which is recommended to test for inducible resistance in staphylococci, streptococcus pneumoniae, and beta-hemolytic streptococci that are erythromycin resistant but clindamycin susceptible. The D test detects resistance by observing whether the zone of inhibition around a clindamycin disk is flattened near an erythromycin disk. A positive result indicates inducible resistance and that clindamycin treatment may fail in vivo due to selection of resistant mutants. The procedure and interpretation of the D test is described along with its limitations and clinical significance when evaluating clindamycin susceptibility.




































































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)





![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)







![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)



